
Summary
More than one third of the population of Kabwe, Zambia— over 76,000 people—live in lead-contaminated townships. Studies estimate that half of the children in these areas have elevated blood lead levels that warrant medical treatment.

Kabwe, the capital of Zambia’s Central Province, was home to a lead mine from 1904-1994. During that period, smelter fumes covered much of the surrounding soil with lead dust. The mine, which opened while Zambia was a British colony, was owned and operated by British companies until 1970, when the Zambian government nationalized the mining industry. The government closed the mine in 1994 and privatized its assets the following year. Since then, seasonal flooding and windblown dust from the mine dump, as well as ongoing small-scale mining, have worsened the contamination.
Twenty-five years after the mine closed, high lead levels, exceeding international standards, remain in the soil and dust around the former mine, particularly in the townships of Kasanda, Makandanyama, Chowa, Mutwe Wansofu, and Makululu in Kabwe. The former mine area itself still hosts tailings and other waste from the mine and smelter, including a large waste dump known locally as “Black Mountain,” and has become a site for artisanal and small-scale mining.
Children in Kabwe are especially at risk because they are more likely to ingest lead dust when playing in the soil, their brains and bodies are still developing, and they absorb four to five times as much lead as adults. The consequences for children who are exposed to high levels of lead and are not treated include reading and learning barriers or disabilities; behavioral problems; impaired growth; anemia; brain, liver, kidney, nerve, and stomach damage; coma and convulsions; and death. After prolonged exposure, the effects are irreversible. Lead also increases the risk of miscarriage and can be transmitted through both the placenta and breastmilk.
Lead pollution is invisible, as lead-contaminated soil appears no different from uncontaminated soil. Many of the health effects of lead also go unnoticed, given that long-term harm to internal organs or brain development may not manifest in immediate symptoms. In Kabwe, even the most severe effects from lead are hidden. Although there are limited records of children’s hospitalization and death from lead poisoning from the early 1970s, there are no recent records, as Zambia’s health system does not track such cases.
Given that the contamination is still present a quarter century after the mine closed, this report documents the impact of lead on children’s rights and the Zambian government’s response to the crisis. Human Rights Watch conducted three field research missions to Zambia between June 2018 and April 2019, interviewing government officials, civil society representatives, families impacted by the contamination, and others to assess the government’s approach and its implications for children’s rights to health, a healthy environment, education, and play.
We found that government efforts to address the lead pollution have been far from adequate. From 2003 to 2011, the World Bank funded the Copperbelt Environment Project (CEP) intended to clean up the lead in affected townships and address its health impacts. The government failed to adopt an effective model for achieving the project’s goals and has not done enough to address the pollution since then either. Rather than design and implement a comprehensive remediation program, the government’s measures have relied on grass planting at homes and schools, some topsoil replacement, and community education on dust reduction. The government’s focus on grass-planting as a home remediation measure proved to be unsustainable once the CEP ended. The government has also failed to address other sources of lead contamination, including road dust. As a result, tens of thousands of families are still exposed to lead on a daily basis.
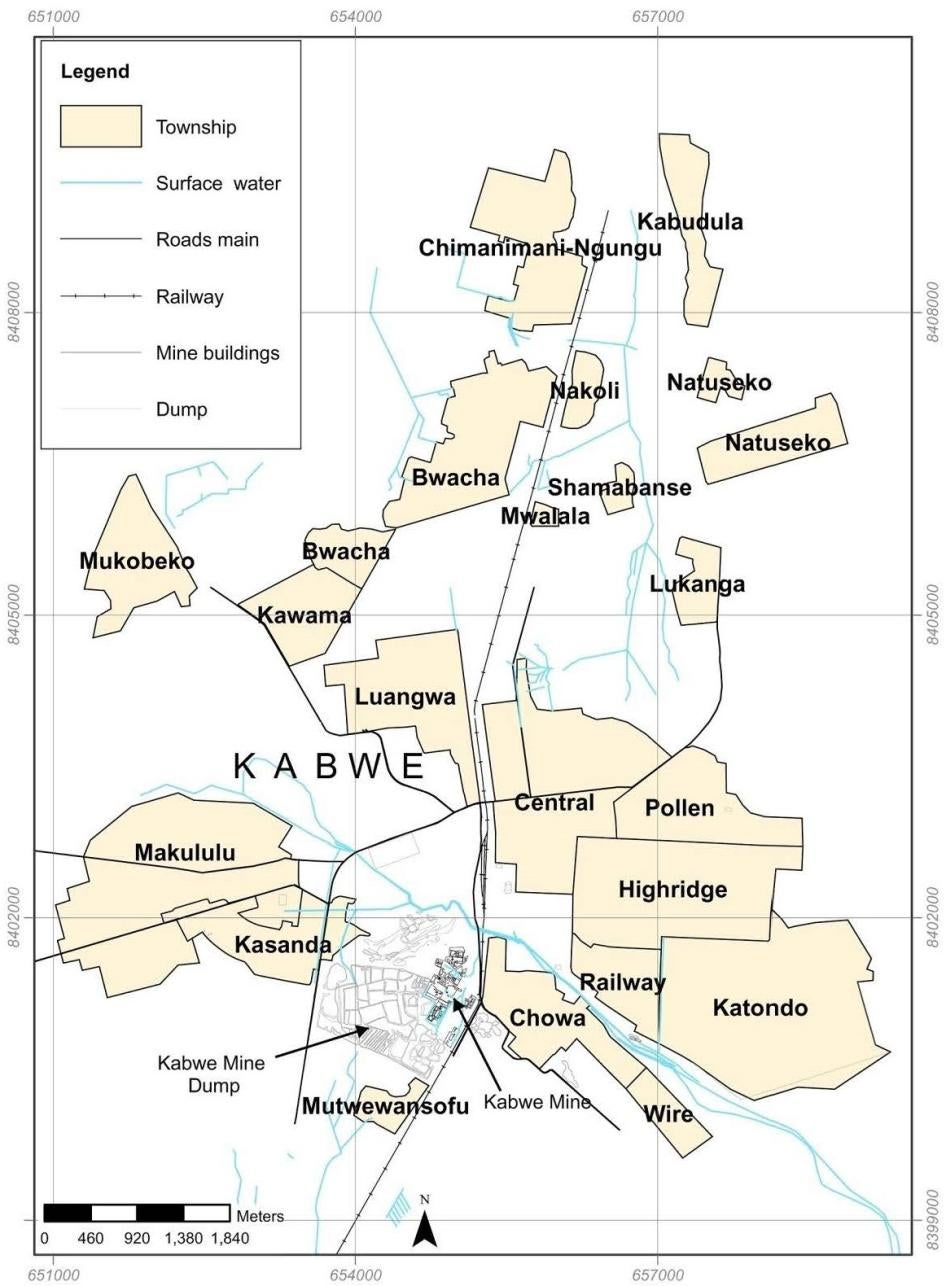
This map of Kabwe includes the lead-affected townships of Makululu, Kasanda, Chowa, Waya (spelled “Wire” here), and Mutwe Wansofu. Makandanyama, another lead-affected township, is not labeled on this map but can be found directly beneath Makululu and Kasanda on other maps.
Joseph Makumba/ZCCM-IH, reproduced in Owen Chasoba Chilongo, “Understanding Kabwe’s Lead Pollution” (M.A. thesis, University of Texas at Austin, 2014), p. 15, https://repositories.lib.utexas.edu/bitstream/handle/2152/28226/CHILONGO-THESIS- 2014.pdf?sequenAlthough the government provided medical care to over 2,800 children under age 7 as part of the CEP, there was no sustained testing and treatment for Kabwe residents. At time of writing, government-run health facilities in Kabwe had no chelation medicine for treating lead poisoning or lead test kits in stock, with no health database to track cases of lead-related hospitalization or death. Education for children with disabilities or learning barriers is a country-wide challenge in Zambia, and in Kabwe, the disability screening process does not even investigate lead-related causes. Large waste piles at the old mine site and ongoing small-scale mining continue to pose health risks. Current plans by private companies to process the mineral waste at the former Kabwe mine could present further risks to human health and the environment, if not adequately regulated and overseen by the government.
Human Rights Watch research found that lead contamination in Kabwe has a disproportionate impact on the poor for at least three reasons: undernourishment increases the amount of lead the body absorbs, lead dust is a particular hazard in informal settlements, and the water required to maintain grass and reduce dust is expensive for community members.
In December 2016, the government launched a five-year World Bank-funded project, the Zambia - Mining and Environmental Remediation and Improvement Project (ZMERIP), that is slated to offer much-needed environmental cleanup, along with a new round of testing and treatment. However, more than two years after the project was launched, there has been no remediation, testing, or treatment. The government informed Human Rights Watch in July 2019 that at least some of the project's cleanup and health interventions would begin before the end of 2019.
Human Rights Watch is concerned that that the project will not address the full scope of lead poisoning and contamination. The project is intended to carry out remediation to reduce lead exposure in at least three townships; the government has indicated that it does not have enough resources to address the full scale of the contamination in homes and compounds, schools, play areas, health centers, and other public spaces. Road paving is not planned as part of the project although unpaved roads present a significant contamination risk because they are covered with lead dust.
With regards to health, the project plans to test and treat at least 10,000 people, including children and pregnant women. Given the total number of residents in lead-affected areas, Human Rights Watch is concerned that the project will not reach all affected children and adults.
Human Rights Watch shared its key findings with the Zambian government prior to the report’s publication. The Ministry of Mines and Minerals Development sent a written response (Appendix I) with more details on their plans under ZMERIP. The response emphasized that the resources available under the current World Bank-funded project could not address all the issues related to lead pollution in Kabwe, and that the government would continue to mobilize resources to reduce lead pollution.
Given that Kabwe residents continue to be exposed to high lead levels, the Zambian government should adopt a sustainable and comprehensive plan for addressing the impact of lead contamination. The government should ensure that its remediation design allows for long-term containment or removal of lead hazards and that it addresses the full scope of the contamination in affected areas. Without remediation, anyone who receives treatment for lead poisoning will be re-exposed to lead when they return home. Initial rounds of testing and treatment should prioritize those who are most vulnerable to lead poisoning, including children under age 5 and pregnant and breastfeeding women. All children and adults in Kabwe, however, should be eligible for testing and treatment. Going forward, the government should also design and implement a comprehensive remediation and reclamation plan for the former Kabwe mine itself to address the long-term contamination risk posed by the mine waste.
The Zambian government has a responsibility to clean up the lead and ensure access to appropriate health services. Its insufficient action on lead pollution has resulted in violations of Kabwe residents’ rights to health, health information, and a healthy environment. Given children’s particular vulnerability to lead poisoning and their heightened protection needs, the ongoing contamination and the failures of the health system have had a devastating impact on children’s rights.
Recommendations
To the Government of Zambia
- Acknowledge full responsibility for remedying the ongoing harms caused by the now-defunct Kabwe mine.
- Develop a program for sustainable, comprehensive lead remediation, testing, and treatment in Kabwe. The program should establish a fund to support ongoing nutrition and health care needs for long-term lead-affected residents of Kabwe.
To the Ministry of Mines and Minerals Development
- Conduct a thorough environmental assessment of current lead levels in Kabwe soil, dust, air, crops, and water, as well as other possible exposure pathways, to identify priority areas for remediation under the current World Bank-funded project, and publish this data.
- Ensure that the remediation of contaminated hotspots under the current World Bank-funded project and any other efforts are both comprehensive and sustainable.
- Develop a remediation plan that will allow for long-term containment or removal of lead hazards, such as removing contaminated soil or covering with barrier cloth.
- Invite all households in contaminated townships to participate in the voluntary remediation program to clean both yards and home interiors.
- Remediate contaminated schools, play areas, health centers, and other public areas.
- Pave roads in contaminated townships to reduce dust.
- Conduct regular monitoring of soil and air lead levels in Kabwe, and publish the results.
- Ensure that small-scale mining activities at and around the former Kabwe mine are closely monitored and that laws and regulations on mining and the environment are enforced.
- Inform miners about precautions they should take to protect themselves and their families from lead.
- Develop alternative economic opportunities for artisanal and small-scale miners.
- Together with the Ministry of Labour and Social Security, assist children to transition out of small-scale mining operations in Kabwe and into schools and vocational training. Ensure that there is ongoing monitoring of child labor in small-scale mines.
- Develop and implement a comprehensive and sustainable solution for the remediation and reclamation of the former Kabwe mine, such as the capping or removal of waste piles.
- Publish all environmental liability agreements developed at the time of mine privatization.
To the Kabwe Municipal Council
- Publish existing data on lead levels in soil, air, and elsewhere in the environment in Kabwe.
- Work with the Ministry of Mines and Minerals Development to ensure that the remediation of contaminated hotspots under the current World Bank-funded project and any other efforts are comprehensive and sustainable.
- Ensure regular, broad, and meaningful public consultation and participation in the development, implementation, and monitoring of remediation efforts. Include dedicated measures that facilitate the participation of groups that may face specific impacts or that are marginalized, such as women, youth, children, the elderly, and people with disabilities.
To the Kabwe District Health Office
- Ensure that all children and adults in Kabwe are given access to free testing and, as appropriate, free treatment for lead poisoning. Undertake regular monitoring of blood lead levels, iron deficiency, neurodevelopment, nutrition, and other relevant indicators. Ensure that all treatment, especially chelation therapy, coincides with remediation; without remediation, patients will be re-exposed to lead when they return home.
- Ensure that the initial round of testing and treatment reaches the most vulnerable members of Kabwe’s population, including all children under age 5 and pregnant and breastfeeding women.
- Ensure that children who were previously tested and found to have elevated lead levels are given access to follow-up testing, treatment, and monitoring.
- Ensure that hospitals and health centers in affected areas are adequately resourced and equipped, including with test kits, nutritional supplements, and chelation medicine and that staff can administer tests, counsel patients on the results, and administer treatment.
- Ensure that everyone tested receives the written results of such tests in a language they understand.
- Provide support for women with elevated blood lead levels during pregnancy and after delivery, including breastmilk alternatives (i.e., infant formula) for women with elevated blood lead levels. Ensure that breastmilk alternatives are targeted and do not disturb general community norms around breastfeeding. Provide specialized care for infants born to women with elevated blood lead levels.
- Train more community health workers.
To the Ministry of Health
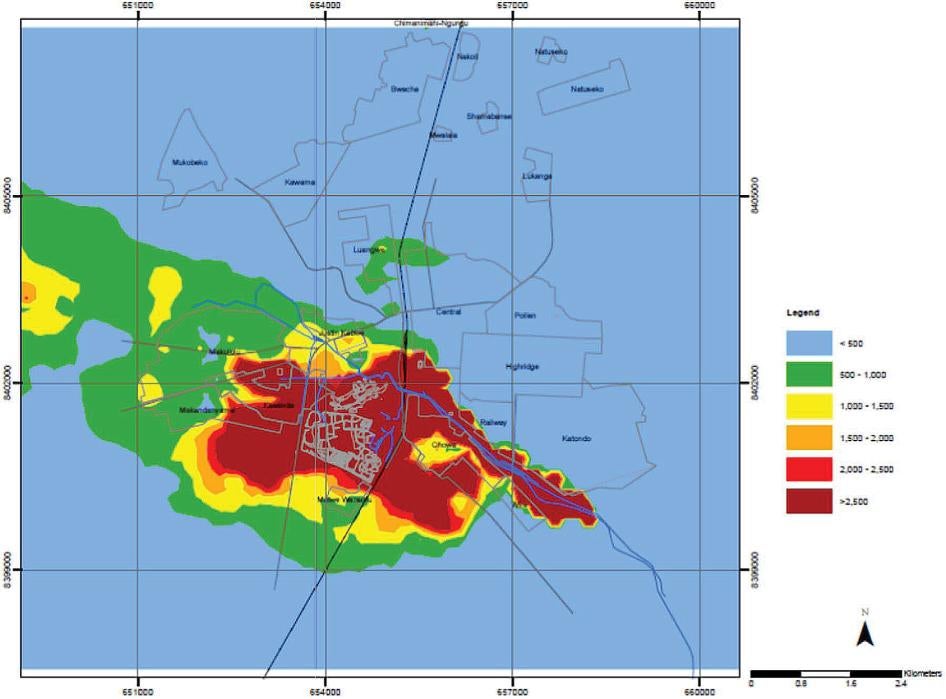
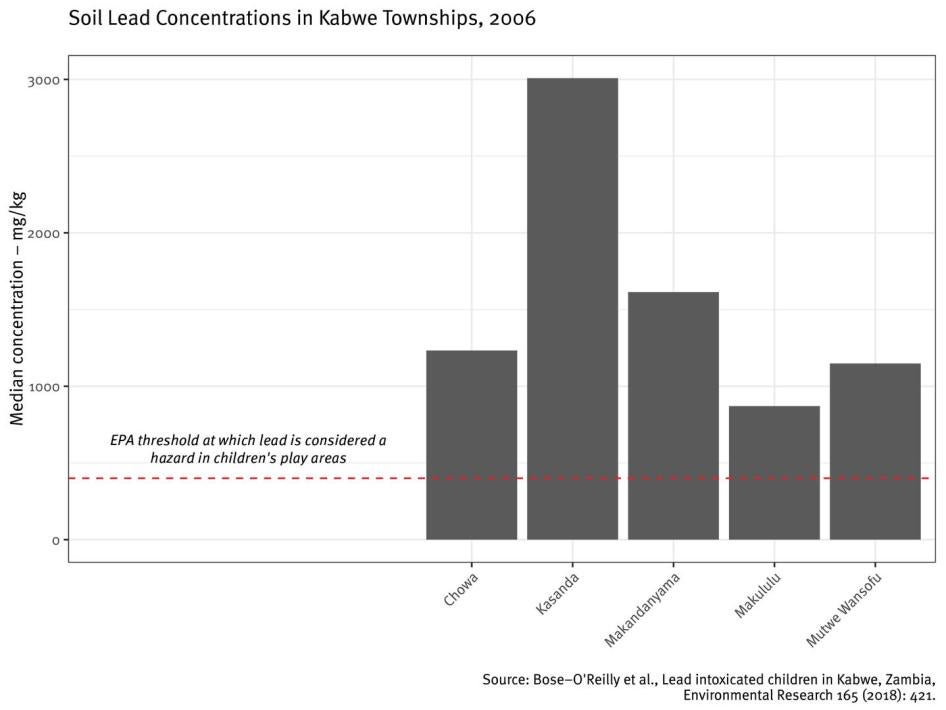
Lead in Surface Soil, Copperbelt Environment Project Soil Sampling Results, 2006. This map, produced by the Kabwe Scoping and Design Study (KSDS) of the Copperbelt Environment Project, is an interpolated distribution of lead in soil based on a district and township survey. This means that soil samples were taken at individual points throughout Kabwe, and the surveyors used a mathematical model to estimate lead concentrations across the whole district. The United States Environmental Protection Agency (EPA) considers lead a hazard in children’s play areas at or above 400 mg/kg.
Stephan Bose-O’Reilly et al., “Lead intoxicated children in Kabwe, Zambia,” Environmental Research 165 (2018): 420, doi: 10.1016/j.envres.2017.10.024.- Ensure health workers at all levels of the public health system are trained on lead poisoning detection and prevention, testing, post-test counseling, treatment, and patient confidentiality.
- Track lead poisoning in the Health Management Information System (HMIS) or develop a separate database for Kabwe to track cases of lead poisoning, including lead-related hospitalization and mortality.
- Update the Zambia Essential Medicine List to include chelation medicine.
To the Zambia Environmental Management Agency
- Conduct an environmental impact assessment of small-scale mining on the site of the defunct Kabwe mine, and ensure that small-scale mining only takes place if it complies with all laws and regulations that protect human health and the environment.
- Conduct a new environmental impact assessment of plans by Jubilee Metals Group to recover lead, zinc, and vanadium from tailings and slag in Kabwe.
- Ensure that any future business undertakings, including re-mining, respect human rights and neither contribute to further lead contamination nor undermine efforts at remediation.
To the Ministry of General Education and the Kabwe District Education Board
- Ensure inclusive education and reasonable accommodations for children with disabilities and learning barriers.
- Integrate environmental education on lead into the school curriculum in Kabwe, and ensure teachers receive additional training to understand how lead can affect learning.
- Instruct the District Assessment Centre to request lead tests for children with disabilities.
- Ensure schools have sufficient numbers of adequately trained teachers to provide learning support while addressing large class-room sizes.
To the World Bank
- Promote regular community engagement and information-sharing under the Zambia - Mining and Environmental Remediation and Improvement Project (ZMERIP).
- Encourage the Zambian government to ensure that key goals for testing, treatment, and remediation are met under ZMERIP in a timely manner.
To Donor Countries and Relevant UN Agencies, such as the International Labor Organization (ILO), United Nation’s Children Fund (UNICEF), World Health Organization (WHO), and United Nations Environment Programme (UNEP)
- Support the efforts of the Government of Zambia and civil society actors to address lead poisoning in Kabwe.
To UN Special Procedures and Treaty Bodies
- Monitor the impact of lead in Kabwe on children’s rights, the right to health, the right to a healthy environment, and the right to a quality, inclusive education.
- Monitor the progress of health and remediation efforts in Kabwe. If progress is poor, consider further measures to effectively advocate for change.
- Monitor the Zambian government’s implementation of its international obligations in relation to lead contamination and children’s rights, such as the Convention on the Rights of the Child and the International Covenant on Economic, Social and Cultural Rights. Urge the government to ensure that it complies with these obligations.
To the African Commission on Human and Peoples’ Rights and Its Working Groups on Extractive Industries, Environment and Human Rights Violations; Economic, Social and Cultural Rights; and Rights of People with Disabilities
- In future research undertakings, missions, or statements on Zambia, address the impact of lead contamination on children’s rights in Kabwe.
Methodology
This report is based on field research by Human Rights Watch in June and November 2018 and April 2019 in Kabwe, Zambia, and the capital, Lusaka.
Given lead’s particular dangers for children, Human Rights Watch set out to assess how the government’s approach to lead cleanup, testing, and treatment has affected children’s rights, 25 years after the closure of the Kabwe mine.
Human Rights Watch interviewed 44 parents and other guardians and 35 children between the ages of 6 and 16 in five townships around the former Kabwe mine where children have been found to have elevated blood lead levels: Chowa, Makululu, Waya, Railway, and Katondo. Most interviews were conducted in the first three townships. In addition, we interviewed 20 adults and 3 older children (ages 16 to 17) working as small-scale miners at the old mine site. We conducted 11 discussions in groups of four or more with over 100 individuals, including parents, children, young adults, teachers, and miners, to learn more about life in lead-affected townships. These included meetings with 10 members of a youth environmental group; about 45 teachers at a public school; three groups of small-scale miners, including anywhere from 10 to 40 miners; and two groups of fewer than 10 parents and other adults in lead-affected townships.
Human Rights Watch researchers also interviewed community members, including school headteachers, teachers, nurses, community health workers, local councilors, and Ward Development Committee members. In addition, researchers interviewed municipal, district, provincial, and central government officials from several ministries and bodies. These included officials from the Ministry of Mines and Minerals Development; Ministry of Health; Ministry of Youth, Sport, and Child Development; Ministry of General Education; Zambia Environmental Management Agency (ZEMA); Human Rights Commission; and the Kabwe Municipal Council. We also met with representatives of the World Bank; Japan International Cooperation Agency; United States Agency for International Development; the German, British, and Canadian governments; and independent civil society organizations working on environmental issues and children’s rights in Zambia.
We also conducted interviews by telephone or in person with experts on lead as it relates to children’s health, environmental health, occupational health, and remediation.
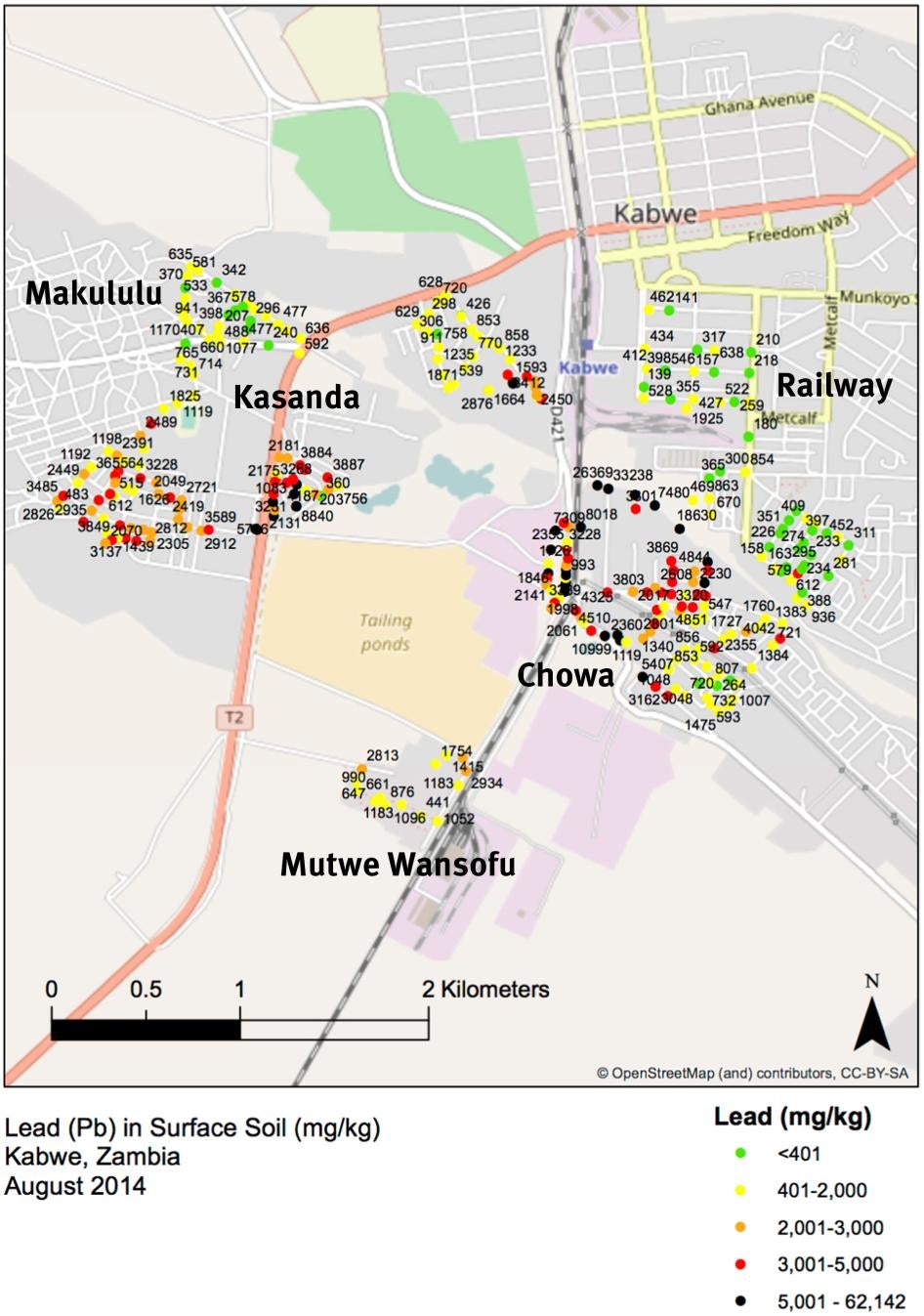
Lead in Surface Soil, Pure Earth Soil Sampling Results, August 2014. This map, produced by the nongovernmental organization Pure Earth, shows the results of soil sampling taken at 339 locations around the former Kabwe mine in 2014. The U.S. EPA considers lead a hazard in children’s play areas at or above 400 mg/kg. Source: in Bose-O’Reilly et al., “Lead intoxicated children in Kabwe, Zambia,” p. 420. Township names were added by Human Rights Watch.
in Bose-O’Reilly et al., “Lead intoxicated children in Kabwe, Zambia,” p. 420. Township names were added by Human Rights Watch.Human Rights Watch conducted most of the interviews with parents and guardians, children, and miners in Bemba, the main local language in Kabwe, with translation into English. Interviews with government officials, representatives of civil society organizations, and other community members were conducted in English.
Most interviews were conducted privately, one-on-one, in quiet places within the affected townships, such as under trees or behind houses. Each individual interview lasted approximately twenty minutes to one hour.
Human Rights Watch also reviewed secondary data sources, including laws, government documents, reports from nongovernmental organizations (NGOs) and research institutions, and maps.
Interviewees did not receive any compensation; they were informed of the purpose of the interview, its voluntary nature, and the ways in which the information would be used. They provided oral consent to be interviewed and were informed that they could decline to answer questions or could end the interview at any time. Where appropriate, Human Rights Watch provided contact information for organizations that could provide social support or other services.
Some parents and guardians shared information about children’s blood lead levels. The specific blood lead levels provided in this report are solely based on the statements of parents, guardians, or Human Rights Watch partners, based on their recollections. Human Rights Watch was not able to confirm the lead levels referenced in the report for individual children. For that reason, Human Rights Watch cannot guarantee the accuracy of each precise level stated. The same is true for the age at which the child was tested and the year of testing.
Human Rights Watch has used pseudonyms for community members interviewed to protect their privacy.
On the advice of Ministry of Health officials, Human Rights Watch wrote the Kabwe District Medical Officer requesting permission for a meeting. The letter was addressed to the Permanent Secretary of the Ministry of Health in November 2018. Human Rights Watch sent a follow-up letter in February 2019. Both letters went unanswered.
In June 2019, Human Rights Watch wrote the World Bank inviting staff to comment on our key findings related to World Bank-funded projects in Kabwe. The World Bank sent a response, which Human Rights Watch references in this report.
In July 2019, Human Rights Watch shared its key findings with Zambian government officials. The Ministry of Mines and Minerals Development sent a written response (Appendix I) with more details on the government’s plans under ZMERIP.
I. Background
Mining in Kabwe
In 1902, lead, zinc, and vanadium deposits were discovered in Kabwe, then known as Broken Hill. Zambia was still a British colony. The Rhodesian Broken Hill Development Company, registered in London, opened the mine in 1904. By 1927, the Anglo American Company of South Africa obtained a controlling interest in the company.[1]
As early as 1916, there were reports that the mine’s management lacked the technology and personnel to mitigate toxic lead fumes. In 1936, miners asked for compensation for workers who could not work because of sickness from the lead fumes. Doctors’ certificates from the time revealed that smelter workers often experienced lead poisoning.[2]
In 1970, six years after Zambia became an independent nation, the Zambian government nationalized the mining industry.[3] In 1994, the government-owned Zambia Consolidated Copper Mines Limited (ZCCM) closed the mine, where operations were no longer profitable, and privatized ZCCM’s mining assets the following year. When privatization was complete in 2000, the company became ZCCM Investment Holdings (ZCCM-IH).[4]

Decades of mining in Kabwe took a toll on the surrounding environment and the health of its residents. Smelter fumes, windblown dust, and seasonal flooding of the mine canal left high concentrations of lead in the soil and dust at the mine and in residential areas surrounding it.[5] Studies have found unsafe levels of lead in soil, dust, crops, and livestock in Kabwe.[6] One study found that surface water near the former mine was contaminated, but groundwater was not.[7] Another study found lead levels above World Health Organization guidelines in one well in Kabwe, out of 13 wells tested.[8] A geologist told Human Rights Watch that uncovered shallow wells in lead-affected townships could be contaminated with suspended lead particles.[9]
The former mine area itself still hosts tailings and other waste from the mine and smelter, including a large waste dump known locally as the “Black Mountain,” and has become a site for artisanal and small-scale mining.
After privatization, the government decided that ZCCM-IH should retain all historic environmental liabilities in its new Environment Department, which was turned into a subsidiary called Misenge Environmental and Technical Services Limited (METS) in 2013.[10] This meant that ZCCM-IH, a government-owned company, held the legal responsibility to address the environmental and health impacts of the former mine on Kabwe residents.
While ZCCM-IH has taken some measures to address the effects of lead pollution in Kabwe—described further below—it has not addressed the toxic legacy of the mine in any comprehensive way.
Health Effects of Lead Exposure
Lead is a heavy metal that is highly toxic to humans when ingested or inhaled.[11] The World Health Organization (WHO) maintains that there is no known safe level of lead exposure.[12] Elevated lead levels damage the brain, kidneys, liver, stomach, nerves, and blood cells, which may result in anemia, IQ deficits, reduced attention span, reading and learning disabilities, behavioral problems, hearing loss, impaired growth and visual and motor functioning, anemia, high blood pressure, coma, convulsions, or death.[13] Lead poisoning can often go undetected, as it may not manifest in obvious symptoms.[14]
Since 2012, the United States Centers for Disease Control and Prevention (CDC), the US public health agency whose lead standards are consulted internationally, has considered 5 micrograms/deciliter (μg/dL) or above to be an elevated blood lead level in children.[15]
The US Environmental Protection Agency, which sets standards for environmental regulation, considers lead in soil to be a hazard when it is at, or above, 400 parts per million (ppm)—equivalent to 400 mg/kg—for children’s play areas and 1200 ppm or 1200 mg/kg for non-play areas.[16] The World Bank has relied on these standards when describing soil contamination in Kabwe.[17]
Children are especially at risk of lead poisoning because they often put their hands in their mouths or play on the ground, which increases their likelihood of ingesting or inhaling lead in dust and dirt, because their brains and bodies are still developing, and because they absorb four to five times as much lead as adults.[18] The potential damage of lead poisoning in children is high because lead affects the development of their nervous and digestive systems.[19]
Among pregnant women, lead exposure can result in stillbirth, miscarriage, and low birth weight and can negatively affect brain development of a fetus.[20]
Symptoms of lead poisoning are often not diagnosed as such. Its adverse health effects can be irreversible.[21] Generally, people exposed to lead at a low level do not display symptoms of poisoning. The severity of symptoms increases with prolonged exposure.[22]
Globally, lead exposure is estimated to account for 540,000 deaths annually, with the highest burden in low- and middle-income countries. Lead exposure accounts for 64 percent of the global burden of idiopathic developmental intellectual disability.[23] Poor and disadvantaged populations are more vulnerable to lead poisoning because undernourishment increases the amount of ingested lead the body absorbs.[24]
A lead expert told Human Rights Watch that good nutrition will never help avoid elevated blood lead levels but can mitigate adverse effects. Calcium and iron compete with lead for sites within the body, so increased intake of calcium- or iron-rich foods can help bring down lead absorption rates.[25]
Chelation therapy is the most common treatment for lead poisoning. Chelation medicine attaches to lead and other heavy metals in the bloodstream, forming a compound that is then released in urine. The medicine can be administered orally or through injection.[26] Chelation therapy is only advisable in cases of severe lead poisoning with lead levels greater than 45 μg/dL.[27] Chelation therapy removes lead from the bloodstream to prevent further absorption into the organs and bones, but it cannot reverse all of the health effects of any lead previously absorbed.[28] Chelation therapy will not be effective unless the patient’s environment is remediated. Otherwise, the patient will continue to be exposed to lead contamination.[29]
The Zambian Health System
Despite being classified as a lower middle income country, Zambia faces relatively high rates of poverty and malnutrition. Zambia’s per capita GDP is only slightly lower than the sub-Saharan African average, yet, as of 2015, 57.5 percent of Zambians lived in poverty, compared with a regional average of 41 percent.[30] Malnutrition affects over half of all children. The 2013-2014 Zambia Demographic Health Survey found that 15 percent of children under age 5 were underweight, 40 percent were stunted (signifying chronic malnutrition), and 6 percent were wasted (signifying acute malnutrition).[31]
Ninety percent of patients in Zambia are served by the decentralized, publicly funded health system. The remaining 10 percent seek care from nonprofit providers, mining companies, or for-profit providers. The Ministry of Health is responsible for coordination, management, policy development, strategic planning, and resource mobilization. Provincial Health Offices liaise between the national and district levels. District health offices hold primary responsibility for coordinating service delivery in district hospitals and local health centers. Primary health care is delivered by local health centers, staffed by clinical officers, midwives, nurses, and environmental officers. They provide a range of free services, including programs on maternal, newborn, and child health.[32]
Zambia achieved 78 percent availability of essential medicines in 2014, according to the government.[33] The Zambia Essential Medicine List does not include chelation medicine,[34] despite the inclusion of chelation medicine on both the WHO Model List of Essential Medicines[35] and the WHO Model List of Essential Medicines for Children, which set standards for priority medicines in national health systems.[36] A WHO expert committee updates the lists every two years.[37] Zambia also does not yet have its own poison center. From January 2012 to December 2013, Zambia participated in a WHO project aimed at improving poison center capacity in Eastern Africa. The Zambia Environmental Management Agency (ZEMA) obtained funding for the project through the Quick Start Programme of the United Nations Environment Programme. In conjunction with the project, Zambia participated in two multi-stakeholder meetings with other countries in the region, held a national workshop, and drafted plans to establish a national poison center.[38]
The National Health Management Information System (HMIS), a national health database, allows the government to analyze progress on key health issues, such as malaria,[39] but it does not track cases of lead poisoning or lead-related mortality.[40]
Kabwe has twenty-nine health centers and two public hospitals, Kabwe General Hospital and Kabwe Mine Hospital, which serve over 200,000 people. All services offered at the hospitals are chargeable depending on the situation or diagnosis, unless patients are referred from a clinic. Only antiretroviral therapy services and counseling are free.[41] Mine Hospital, which is adjacent to the mine site and the lead-affected townships, is smaller and has a higher fee structure than the General Hospital.[42]
Kabwe Geography and Local Government
The capital of Zambia’s Central Province, Kabwe is a town spanning about 1,570 square kilometers, with a population of over 200,000.[43] The old mine site, which is at the southern end of Kabwe, is about 3 square kilometers, and the whole mine area, including the mine site, plant, and waste (tailings), covers more than 7 square kilometers.[44]
The Kabwe townships closest to the former mine site include Chowa, Kasanda, Makululu, Makandanyama, Mutwe Wansofu, Waya, Katondo, and Railway.[45]
Residential housing patterns and water access vary from one township to the other. The townships of Chowa and Kasanda, for example, are planned settlements, originally built as housing for miners. Houses in these townships have running water and are constructed with concrete bricks. Makalulu, Waya, and Katondo, meanwhile, are unplanned settlements, where houses have thatched roofs, mud brick walls, and mud floors, and most households rely on a combination of communal water taps and well water.[46]
The Kabwe Municipal Council is the local administrative body in Kabwe. Kabwe also has elected councilors from its 27 political wards.[47] Each ward has a Ward Development Committee, which consists of a group of residents who share recommendations with their ward councilor and the Kabwe Municipal Council based on their assessment of community needs.[48] Townships may encompass multiple wards, and some wards may overlap with more than one township.[49]
Lead Contamination in Kabwe
First Documentation of a Crisis: 1971-1975
The harmful effects of lead on the environment and human health in Kabwe have been documented since the 1970s, including the hospitalization and deaths of children.
Over a 2.5-year period from 1971-1974, 27 children from Kasanda were admitted to Kabwe General Hospital for convulsions and comas and were confirmed to have lead poisoning. Despite receiving chelation therapy, four died, two of them solely because of their lead levels.[50]
In 1975, British researcher A.R.L. Clark published a study documenting these cases along with high lead levels in the soil, air, and vegetation in Kasanda, Chowa, and Makululu, and elevated blood lead levels in infants, children, and new mothers. Clark tested over 600 children in Chowa, Kasanda, and Makululu and 125 newborn infants and their mothers in Kasanda. Clark found a direct correlation between high blood lead levels in newborns and their mothers. Soil lead levels were as high as 9,400 ppm. The period Clark studied is the only time for which lead-related hospitalization and mortality data is available on Kabwe.[51]
Development of a Government Response: 1990-2002
From 1990-1999, six programs—including three by ZCCM—surveyed soil lead concentrations, and all found high levels of contamination. In 1994, ZCCM launched a blood testing program, focusing on Kasanda and Chowa, which tested 866 children and adults and found elevated blood lead levels across all age groups and the highest levels among children ages 0-5.[52]
ZCCM conducted subsequent blood lead testing programs from 1996-1997 and 1999-2000, administered chelation therapy, provided clean topsoil to households in Chowa to cover the contaminated soil, and gave families tips for reducing lead exposure in the home. A 2002 World Bank-funded environmental assessment deemed the health intervention program “fraught with problems” and “inadequate for the need” and characterized the soil cover as only “the absolute minimum that could be considered adequate.” The environmental assessment team found that the clean topsoil had already begun to erode in some areas, re-exposing the lead-contaminated soil.[53]
Copperbelt Environment Project: 2003-2011
Under the World Bank-funded Copperbelt Environment Project (CEP), the Zambian government undertook a number of steps to address the lead pollution in Kabwe.[54] The project included environmental remediation, testing, and treatment. Ultimately, these efforts proved insufficient. The government did not adopt a comprehensive remediation program and was thus unable to achieve a significant reduction in lead exposure for most residents of lead-contaminated townships.
As part of its remediation efforts, the government cleaned the Kabwe Canal to reduce the risk of lead recontamination through seasonal flooding. It removed mine waste material from some residential areas.[55] It removed topsoil and planted grass and trees in the yards of 3,100 households. The government also planted grass at schools, including those closest to the mine plant area and others in Kasanda, Makandanyama, Mutwe Wansofu, Makululu, and Luangwa.[56] It built new water infrastructure and subsidized water rates to make it less difficult for residents to maintain the new vegetation.[57]
The government also constructed 11 community parks in Chowa, Kasanda, Katondo, Mutwe Wansofu, MaKandanyama and Makululu and rehabilitated an additional one, but the World Bank’s project assessment noted that all but two of the parks were later vandalized or had equipment broken.[58]
From 2007-2010, the project supported an Integrated Case Management program, which conducted blood lead testing of about 5,000 children below age 7 at local health centers and provided treatment (nutritional supplements—including milk, soya, and blood tonic—or chelation therapy) to about 2,800 of the children tested.[59] Children whose blood lead levels were found to exceed 65 μg/dL (Class 5) were given chelation therapy. Children whose blood lead levels were 45-64 μg/dL (Class 4) and 20-44 μg/dL (Class 3) received nutritional supplements. Children whose lead levels were 10-19 μg/dL (Class 2) were put under observation.[60]
As a result of inadequate environmental remediation, the project failed to meet its objective of reducing children’s blood lead levels in Chowa, Kasanda, Katondo, Mutwe Wansofu, MaKandanyama and Makululu to an interim level of 25 μg/dL and ultimately to 10 μg/dL.[61]
Human Rights Watch reached out to the World Bank regarding the CEP’s failures, and the World Bank stated that they recognized the project’s shortcomings, which they said were well-documented in the Bank’s evaluation reports.[62] The World Bank said that the CEP “was challenged during implementation by slow progress on the enabling environmental and mining policies framework, weak capacity of the implementing agencies and lack of institutional continuity.”[63]
Lack of Sustained Government Efforts: 2012-2019
Independent researchers have confirmed that the lead contamination in Kabwe remains severe, and children’s blood lead levels far too high. Their work underscores the inadequacies of the government’s efforts to address the problem. Following the end of funding for the CEP and the consequent closure of the project in 2011, the government has not done enough to address the ongoing contamination or children’s elevated blood lead levels. Some NGOs and others have taken steps to reduce the contamination, providing possible models the government could scale up in future efforts.
After the closure of the CEP in 2011, ZCCM-IH continued to administer the CEP’s testing and treatment program for children under 7.[64] This time, however, there was no chelation medicine left for children with the highest blood lead levels, and there was no ongoing cleanup effort to reduce the environmental threat.[65] METS, the newly created ZCCM-IH subsidiary, took over the program in 2013 and continued to conduct regular blood lead testing of children through 2014 and some re-testing through 2016 until test kits ran out.[66] In its 2017 annual report, ZCCM-IH reported that it had reached 3,031 children during the year at Chowa, Kasanda and Makululu Health Centres, although Human Rights Watch was unable to determine how many how many of these children were re-tested, given the limited number of test kits available at the time.[67]
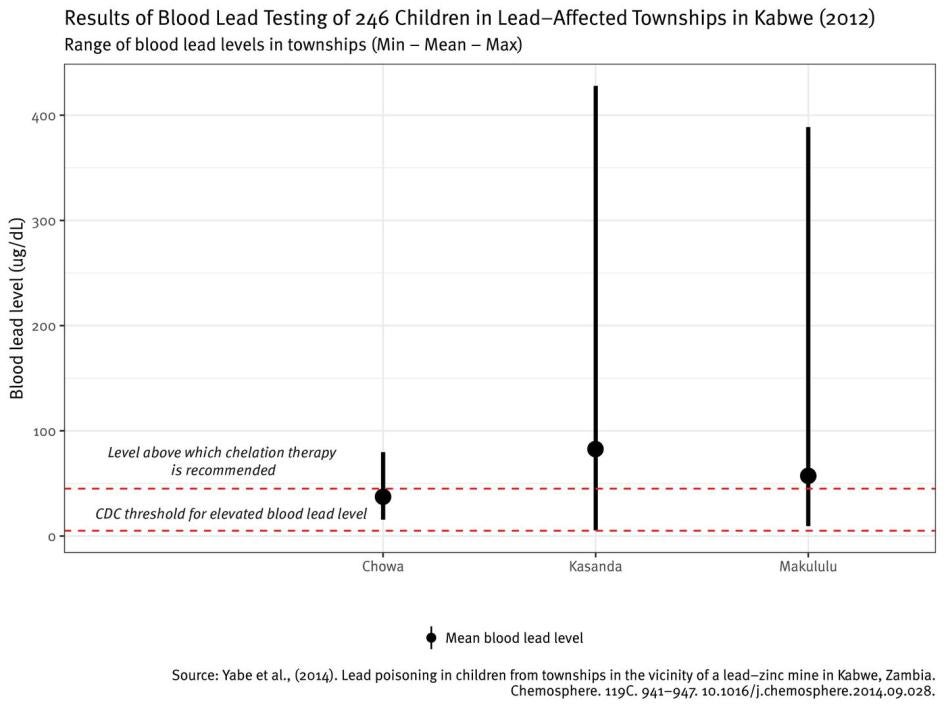
In May-June 2012, researchers at the University of Zambia, Hokkaido University in Japan, and the Zambian Ministry of Health conducted blood lead testing of 246 children under age 7 at health centers in Chowa, Kasanda and Makukulu and found “alarming” levels. All children had blood lead levels greater than 5 μg/dL, suggesting the need for continued monitoring and follow-up testing. Eight children were found to have blood lead levels over 150 μg/dL.[68] A lead expert told Human Rights Watch that at or above this level, about half of children would be expected to die or have seizures or comas.[69]
In July 2014, Pure Earth, an international nongovernmental organization, found that the soil in townships surrounding the mine remained highly contaminated, with concentrations as high as 62,142 mg/kg and a geometric mean of 1,470 mg/kg, far above the threshold of 400 mg/kg.[70] Pure Earth tested 196 children ages 2-8 and found a mean blood lead level of 48.3 μg/dL, which itself was above the level for medical intervention of 45 μg/dL.[71]
In 2015, Pure Earth partnered with the regional organization Environment Africa, the Kabwe Municipal Council, and a staff of local contractors to launch a pilot home and yard remediation program in Chowa. The program remediated 120 households before funding ran out in 2017.[72] Environment Africa also founded youth environmental clubs in several public schools, whose members educated their peers and community members about lead.
From 2015-2016, Dr. Samuel Mutiti, a US-based geologist, led a research team that collected soil samples at eight schools in Kabwe, five near the mine and three as a control group. He thereafter organized a crowdfunding campaign to remediate a severely contaminated school, raising over $3,000 so far. In partnership with local education authorities, he has begun building a fence around the school to keep out dust and reduce foot traffic and has begun covering lead-contaminated soil with clean soil.[73]
In May 2016, the Japan International Cooperation Agency (JICA) and the University of Zambia, in partnership with the Zambian government, launched the Kabwe Mine Pollution Amelioration Initiative (KAMPAI Project), a multi-disciplinary, five-year research project intended to identify the environmental, health, and socioeconomic effects of lead in Kabwe, as well as possible remediation strategies. The project has undertaken its own blood lead testing of select children and adults in Kabwe, aiming to test four family members each from 25 households in each of Kabwe’s 40 census areas, and will oversee the blood lead testing that occurs under the government’s new World-Bank funded project.[74]
In December 2016, the Zambian government and World Bank launched the Zambia - Mining and Environmental Remediation and Improvement Project (ZMERIP) to follow up on the CEP and address environmental health risks in highly polluted areas in Kabwe and the Copperbelt, an adjacent province.[75] The five-year project includes plans for remediation, testing, and treatment in Kabwe and has the potential to offer a more sustainable solution to Kabwe’s lead problem. At time of writing, however, no remediation, testing, or treatment had commenced. The Ministry of Mines and Minerals Development informed Human Rights Watch that at least some cleanup and health interventions under the project would begin before the end of 2019.[76]
II. Findings
In June and November 2018, Human Rights Watch visited five townships in Kabwe where children have been found to have elevated blood lead levels: Chowa, Makululu, Waya, Railway, and Katondo. We interviewed parents and guardians of children with elevated lead levels to find out what kind of cleanup, testing, and treatment efforts the government had carried out in the years after the Copperbelt Environment Project (CEP) ended in 2011. We interviewed local education officials, school headteachers, teachers, and students to learn about the extent of government efforts to examine contamination in schools and to ensure quality, inclusive education for children with disabilities. We also interviewed small-scale miners at the site of the former Kabwe mine about the hazards of their work, the precautions they take to reduce lead exposure, and their reasons for seeking a livelihood there. Finally, we asked community members, including children, what they would like the government to do to address the lead contamination, especially in light of the current World Bank-funded government project.
We found that the CEP’s remediation model of grass planting at homes and schools proved unsustainable when the project ended, and dust from unpaved roads remained an environmental hazard. The government’s efforts to reduce lead exposure since the end of the CEP largely consisted of sharing dust reduction tips that community members struggled to carry out. Government testing and treatment efforts were limited and inconsistent in the years since the CEP ended. At time of writing, government-run health facilities in Kabwe had no chelation medicine or lead test kits in stock, and there was no health database set up to track cases of lead-related hospitalization or death. Inclusive education is a country-wide challenge in Zambia, and in Kabwe, the disability screening process does not even investigate lead-related causes. Finally, large waste piles at the site of the old mine and ongoing small-scale mining both continue to pose health risks.
***
Malaika has lived in a lead-affected township in Kabwe her whole life. She was first tested for lead in 2008, as part of the CEP testing and treatment efforts, when she was around age 1. Her blood lead level was above 65 μg/dL, well above the CDC benchmark of 5 μg/dL. Her grandmother recalled that Malaika had stomach pain at the time, which may or may not have been the result of lead poisoning.
When Malaika was tested again in 2012, after the project ended, her lead levels were still severe—above 45 μg/dL, a sign of the government’s failure to achieve a significant reduction in environmental contamination. According to international standards, children with lead levels as high as Malaika’s should be considered for chelation therapy, and their environmental lead exposure should be mitigated through remediation. By 2012, however, the government had run out of chelation medicine and ceased cleanup efforts.[77] Malaika was instead given nutritional supplements and returned to her contaminated home environment.[78]
Now 11, Malaika spoke about having trouble in school. “When teacher teach [teaches] me, I forget some things,” she said. Both she and her grandmother noted that Malaika’s stomach pain continues today, which, along with the other struggles Malaika described, may or may not be a consequence of lead poisoning. The frightening thing is that the family has no way of knowing. Malaika and her grandmother told Human Rights Watch that sometimes the pain is so hard to bear that Malaika stays home from school. “My stomach troubles me…. Sometimes three days, sometimes one week I don’t go to school,” Malaika said.[79]
***
Malaika is one of thousands of children in Kabwe who have been tested and found to have lead poisoning in the past decade. Thousands more have never been tested but are likely to have elevated levels of lead exposure. Over 76,000 people—more than one-third of Kabwe’s population—live in the contaminated townships of Chowa, Kasanda, Makandanyama, and Makululu alone.[80] Approximately 39,000 children live in those four townships, including some 13,000 children under 5.[81]
Researchers estimated in 2018, based on recent blood lead testing samples, that over 95 percent of children in the townships surrounding the lead mine have elevated blood lead levels, and that about half of them have blood lead levels at which medical intervention (chelation therapy) is recommended.[82]
From parents, guardians, and children in Chowa, Makululu, and Waya townships in Kabwe, Human Rights Watch learned firsthand of 60 cases of children who were tested and found to have elevated blood lead levels since the last large-scale government cleanup efforts ended in 2011. Most of these children were among the several thousand children who were tested and monitored by ZCCM-IH from 2011-2016. Like Malaika, they were simply given nutritional supplements and then sent back to the environment that poisoned them. They reported many symptoms consistent with lead poisoning, including loss of appetite, stunted growth, stomach pain, headaches, weakness, memory issues, and concentration problems.[83] Some parents and guardians said their children had no health problems or only reported symptoms unrelated to lead poisoning.
It is impossible to definitively attribute such symptoms to lead exposure, even where there are documented high blood lead levels. However, the symptoms described are all consistent with the consequences expected from lead exposure. Given the extremely contaminated environment, it is likely that many children have symptoms as a result of lead exposure.
The stories of these children reveal the inadequacies of the government’s past approach to remediation, testing, and treatment. Over the course of the past 25 years, generations of families have been tested, told by ZCCM-IH to suppress dust in their homes, and in some cases, given access to chelation therapy, nutritional supplements, clean topsoil, or grass. Yet none of these interventions have come remotely close to addressing the scope of the contamination and health needs in Kabwe.
The stories of Malaika and other children contain vital lessons for the new World Bank-funded government project. By revealing where past efforts have fallen short, they provide a road map for future government action.
Ongoing Environmental Threat
You see dust is everywhere. It is all over. So this lead it just can’t stop spreading.
—Mother, Kabwe, November 2018[84]
We have too much lead. I would like to go to Ndola.
—Girl, about 5, when asked what was her favorite place in Kabwe, November 2018[85]
The inadequacy of past cleanup efforts has left Kabwe’s affected townships contaminated.
From 2003 to 2006, the CEP found median soil lead concentrations that exceeded safe levels (at or above 400 mg/kg) in townships including Kasanda, Makandanyama, Chowa, Mutwe Wansofu, and Makululu.[86]
The most recent sampling effort across multiple townships, conducted by Pure Earth in 2014, confirmed that contamination remained severe, finding soil lead levels that exceeded international standards in several townships surrounding the former mine, with a geometric mean of 1,470 mg/kg.[87] Pure Earth did not publish data on the average lead levels in individual townships, but their soil sampling map indicated high levels of contamination in Kasanda, Chowa, Makululu, and Mutwe Wansofu. Other townships where children have been found to have elevated blood lead levels, including Waya, Katondo, and Railway, were largely outside of the Pure Earth sampling radius.[88]
Over one-third of Kabwe’s population—Chowa (over 14,000 people), Kasanda (over 15,000 people), Makandanyama (almost 20,000 people), and Makululu (over 27,000 people)—live in four of the most affected townships.[89]
Rather than adopt a comprehensive remediation program, the government’s measures so far have relied on grass planting at homes and schools, some topsoil replacement, and community education on dust reduction. The government’s focus on grass-planting as a remediation measure proved to be unsustainable. The government has also failed to address other sources of lead contamination, including road dust. As a result, tens of thousands of families are still exposed to lead on a daily basis.
Lead Exposure in Homes and Yards
“Here in Kabwe the soil is very polluted…. Our children they [are] just stepping on the soil always.”
—Mother of five, Kabwe, November 2018[90]
“They told us to wash hands, grow grass, but the water is very expensive.”
—Mother of three, age 30, Kabwe, November 2018[91]
Residents continue to be exposed to high levels of lead in Kabwe, revealing the inadequacies of past remediation efforts. Lead can be found in the soil in people’s yards in the areas around the former Kabwe mine, as well as dust outside and within homes. Given the extent of contamination, all residents of Kabwe’s affected townships are at risk of ingesting or breathing in lead dust. Resident who grow crops in contaminated soil or cook outdoors face additional risks.
During the dry season from roughly May to October, lead dust represents a particularly significant hazard for those who ingest or inhale it.[92] When Human Rights Watch visited affected townships in Kabwe, dust was ubiquitous. In one family’s backyard, a rooster shook its wings and became enveloped in a cloud of dust. Dust stuck to children’s hands, faces, and clothes as they played outside on the ground. Passing cars and trucks left a thick haze in their wake.
Although dust is a hazard in all of Kabwe’s contaminated townships, the threat is particularly acute in the informal settlements[93] of Makululu and Waya, where housing is much more exposed to the outdoors than in the formal settlements of Chowa and Kasanda.[94] As a result, children in these neighborhoods are likely to encounter more dust in their homes.
Since the CEP ended in 2011, ZCCM-IH staff have continued to conduct home visits intended to share tips with parents and guardians for reducing lead exposure. But the suggested measures—such as watering grass and washing floors and hands regularly—only provide limited protection against lead.
In addition, families have struggled to implement these recommendations. Many of the families who spoke to Human Rights Watch said they could not afford the water necessary to maintain grass or clean their homes regularly, making re-exposure to contaminated soil and dust inevitable.

Lead contamination in Kabwe therefore has a disproportionate impact on the poor for at least three reasons: undernourishment increases the amount of lead the body absorbs, lead dust is a particular hazard in informal settlements, and the water required to maintain grass and reduce dust is expensive.
Officials from ZCCM-IH and the Ministry of Mines and Minerals Development have acknowledged that water is a huge issue. A local city councilor, the members off a local Ward Development Committee, and two public school teachers echoed these concerns.[95]
In all, 19 community members whom Human Rights Watch interviewed identified the lack of affordable water as an impediment to reducing lead exposure. These community members identified water access as a challenge regardless of whether they relied on running water, communal taps, or well water.[96]
A man who had three grandchildren with elevated lead levels observed that people needed water to keep grass alive and said, “Right now the cost of water is higher than electricity…. It’s horrible. Charges are too high.” Other parents and grandparents echoed these concerns. A grandmother said she had been told to sprinkle water when sweeping, but it was hard to do. When she used more water, the bill would rise steeply.[97]
Other models for home remediation do not depend on water and are therefore more likely to last in Kabwe. For example, the above-mentioned pilot project by Pure Earth and Environment Africa in Chowa combined environmental assessment, yard remediation, house cleaning, community education, and drainage improvements. The yard remediation and house cleaning were voluntary programs, involving the covering of the yard with a barrier cloth and clean soil and then the cleaning of the home with a specialized vacuum.[98] Meanwhile, in Zamfara state, Nigeria, remediation efforts that addressed lead contamination from mining activity focused on removing lead-contaminated soil from residential areas altogether and replacing it with clean soil.[99]
Lead Contamination in Schools, Play Areas, and Health Centers
Inasmuch as you try to make the surroundings green…. We are lacking the recreation facilities. In the afternoon, you can still see children playing [in the dust].
—Teacher, Public School in Kabwe, November 2018[100]
Kabwe’s contaminated townships include public and private schools, play areas, health centers, parks, soccer fields, markets, and places of worship. Past government efforts to clean up public spaces under the CEP focused on rehabilitating areas where children spend the most time, namely schools and play parks. Neither effort proved successful, however. The project planted grass at schools but did not take any sustainable measures to contain the contamination. The project created new, lead-free play parks for children, but nine out of eleven were vandalized.[101]
Schools
There are at least nine public schools and seven private schools, including both primary and secondary schools, in or near Kabwe’s affected townships.[102]
From 2016-2017, a US-based geologist took soil samples at eight Kabwe schools.[103] The only school for which data is currently public is David Ramushu Combined School (pre-school through grade 12) in Kasanda (a township residents also refer to as Mine), where total lead was found to reach 1028.9 ppm and soils on the soccer field had levels of over 6000 ppm, 15 times more than the standard of 400 ppm. The geologist found the school grounds to be so contaminated that he organized independent remediation efforts in 2017.[104] Part of his remediation plans involved grass planting, but he told Human Rights Watch that the cost of water would not be an issue because the school had its own borehole, and he would help them design an irrigation system to utilize it.[105]
Human Rights Watch spoke with headteachers at four other public schools in or near the contaminated areas. None of them knew whether their schools were contaminated. They expressed concern about the hazards of lead and said they would appreciate information on soil levels so that they could ensure a safe learning environment for their students.[106]
One headteacher said:
Of course, if it [the lead] is poisonous, if it can affect our lives, our health, I want to know if we are living with it or if it can affect our health. We have to be worried.[107]
Another headteacher said the school had a lot of dust coming in, but no one had come to test the children or the soil.[108]
Three schools have made their own efforts, relying on school funds or the assistance of the NGO Environment Africa, to plant grass or other vegetation and pave parts of the school grounds to suppress dust.[109]
Play Areas
Playing in Kabwe comes with risks. Children cannot be sure of avoiding lead exposure in their own yards, streets, or schools.
Given the extent of contamination in the townships around the old mine site, children in those areas lack safe spaces to play. Small children have increased hand-to-mouth activity, which makes them particularly vulnerable to ingesting lead soil or dust when they play outside.

A father of three who had recently moved to Railway placed clean soil on his yard and kept his 7-month-old son indoors. He said:
I tried by all means to ensure the child is not eating the soil. I tried to keep the boy enclosed in the house so that he has no exposure.[110]
Unregulated access to the former mine site further endangers children. Intrigued by the massive pile of mine waste, children play there and have done so for decades. In 2002, a government-commissioned environmental assessment noted that two boys had drowned in the past year after going to play in one of the mine pits filled with water. At the time, ZCCM had built a wire fence around the pit, but people had stolen it.[111]
Nearly two decades later, children continue to play on the site. Human Rights Watch spoke to a group of 13 elementary school students, of whom three said they played at the Black Mountain tailings dump. One boy said he slid down the mountain, acknowledging that it was fun but also “dangerous.”[112] In another Human Rights Watch meeting with eleven older children, seven said they had played at the Black Mountain when they were younger.[113]
Spaces intended for play are also contaminated, such as the soccer field at David Ramushu.[114] Human Rights Watch spoke to several young people who called on the government to ensure there were safe play spaces for children, including more lead-free playgrounds.[115]
Health Centers
Human Rights Watch spoke to an environmental health expert who conducted soil sampling at Chowa Health Centre in 2017. The health center, which included a new maternity wing that housed pregnant and breastfeeding mothers, had soil lead concentrations that far exceeded safe levels, ranging from 1,241 ppm to 13,843 ppm.[116] There is no other public data on soil lead concentrations at health centers, but Kasanda Clinic and Mine Hospital are both located within townships found to have extremely high soil lead levels as recently as 2014.[117]

Road Dust
We also want good roads to get rid of the dust that we are inhaling on a daily basis.
—Woman, Miner, Kabwe, November 2018[118]
Even the road should be tarred so that we don’t have exposure to dust.
—Woman, age 37, Kabwe, November 2018[119]
Environmental remediation experts have long identified road dust as a significant contamination risk in Kabwe’s affected townships. As early as 1996, a study conducted for ZCCM-IH emphasized the value of reducing road dust to reduce lead exposure pathways.[120] Similarly, the 2002 World Bank-funded environmental assessment stated:
One area that is relatively easy to address is the reduction of road dust. Ideally, road surfaces would be paved to eliminate dust emissions from traffic…. Priority should be given to the busiest sections of roads that run through the residential areas of Kasanda and Chowa and possibly other areas if they are found to also be contaminated.[121]
Despite this recommendation, the government failed to address the issue of road dust on a large scale. Under the CEP, road paving was not identified as a priority, although a ZCCM-IH representative told Human Rights Watch that the road near Jack and Jill, a private nursery and primary school very close to the old mine site, was paved to reduce the dust from passing vehicles.[122]
More recently, a 2015 study of children’s blood lead levels, co-authored by a representative of the national Ministry of Health, observed that road dust on unpaved roads heightened contamination pathways in Makululu township.[123]
Nine community members with whom Human Rights Watch spoke highlighted the need to pave Kabwe’s roads to suppress lead dust. A mother of two said, “The road should be tarred. The dust raises [rises] and goes back to the house.” A teacher observed that cars passing by on the gravel road kicked up a lot of dust, and another proposed, “If the roads are tarred, it might reduce the dust.” Other community members who called for road paving to reduce contamination included members of a local Ward Development Committee, a former city councilor, and two public school headteachers.[124]
The government’s Road Development Agency has had plans to pave roads in Chowa and Makululu since 2013, but the project has stalled for lack of funds.[125]
Unpaved roads in Kabwe’s contaminated townships can be found throughout the residential areas that the government plans to remediate under its latest World Bank-funded project. So long as roads remain unpaved, road dust risks undermining any new remediation efforts.
Insufficient Access to Testing and Preventive Care
The little one didn’t have the test because they had stopped testing.
—Mother of two, 27, Kabwe, November 2018[126]
Even myself, I want to be tested, to know how I am. Because at times I feel headache, I sweat.
—Grandfather and Former Miner, 65, Kabwe, November 2018[127]
Despite international guidance that children with elevated blood lead levels should receive monitoring and repeat testing, and despite the widespread lead contamination found throughout Kabwe, lead testing itself has not been consistently available.
Several thousand children under 7 were tested from 2011-2016 by ZCCM-IH. Children were tested either at local health centers or at the ZCCM-IH laboratory adjacent to Mine Hospital. They came from the townships surrounding the former Kabwe mine, including Chowa, Kasanda, Makululu, Makandanyama, Mutwe Wansofu, Waya, Katondo, and Railway.[128] All of these townships were found to include at least some children with elevated blood lead levels.[129] Under the program, parents and guardians were not told their child’s precise blood lead level, only the class (i.e., Class 1-5). They were told orally and were not given anything in writing further explaining the lead level.
Despite the widespread need for testing and treatment, ZCCM-IH ran out of test kits in 2016.[130] As a result, most children born after 2016 were never tested for lead. Given that the government’s testing and treatment programs from 2007-2016 only targeted children below the age of 7, many adults, including pregnant women and breastfeeding mothers, never had access to free, government-funded testing.
Human Rights Watch is not aware of any steps being taken to prevent mother-to-child transmission of lead during pregnancy or breastfeeding. If no solid efforts were in fact underway, it would be of particular concern given that a government-commissioned study found that 48 percent of women of childbearing age had lead levels above 10 μg/dL[131] and given the common practice of geophagia (soil ingestion) among pregnant women.[132]
Human Rights Watch spoke to the members of two families where the mothers had high lead levels as children and later had children who could not access testing themselves.
Esther, 60, recalled when three of her children were tested by ZCCM in the 1990s. She was told that they had elevated lead levels but not given the specific results. They were given “medicine tablets.” At the time, all three children complained about headaches. Today, one of Esther’s children has her own son and daughter, who live with Esther. “I need my grandchildren to be tested,” Esther said. “I have two in the house.” Her granddaughter, Natasha, is 4 and has frequent stomach aches and headaches. She has never been tested. Natasha’s brother Charles has never been tested either. Esther said he also complains about abdomen pain and headaches. “Even yesterday he was crying.”[133]
Kasuba, 26, was tested around 2000 by ZCCM-IH and found to be Class 4. She was given milk and soya. Today she has headaches and pain all over her body. Neither of her children, age 6 and 4 months respectively, have been tested. Joshua, her older son, complains of headaches, and his mother said he is forgetful. He has difficulty concentrating in class and leaves his materials at school, coming home with neither books nor pencils. Both her sons could have lead poisoning, Kasuba observed, since she was found to have it herself and since they grew up in the same environment. When Kasuba went to school, she said she understood concepts when the teacher explained them, but remembering them was a problem. No one explained to her that lead could be transmitted through a mother’s milk.[134]
Human Rights Watch also spoke to parents whose older children had been tested and whose younger children had not been tested but said that they exhibited similar symptoms.[135]
Cynthia, a mother of three, said that only her 8-year-old daughter was tested. She was found to be Class 4. Her 6-year-old son was forgetful and would always have headaches, but he was not tested. Her 9-month-old was not tested either.[136]
Adults, too, reported symptoms of lead poisoning and asked Human Rights Watch why the government had not given them access to testing. Cynthia said she sometimes felt very tired and weak herself, but she was not tested when her daughter was.[137]
Inadequate Treatment
They tested our children and found them with lead, but they can’t provide medication.
—Mother, 27, Kabwe, November 2018[138]
Most of the children with lead exposure whose parents or guardians Human Rights Watch interviewed have not had access to proper treatment, due to a lack of chelation medicine and limited stocks of nutritional supplements, such as milk, soya, and blood tonic.
Even when treatment has been provided, treatment efforts have been fraught with problems. Without ongoing cleanup, no treatment program can effectively reduce lead poisoning because patients will be immediately re-exposed.
Lack of Chelation Medicine
Officials at ZCCM-IH told Human Rights Watch that the ZCCM-IH testing and treatment program no longer included chelation medicine after the CEP ended in 2011.[139] Human Rights Watch is not aware of a single individual who received chelation through a government program after 2011. According to Ministry of Health officials and hospital staff, chelation medicine is not currently available at either of Kabwe’s two public hospitals.[140]
Human Rights Watch interviewed the parents or guardians of 28 children who were found to have lead levels above 45 μg/dL, the threshold at which chelation therapy is advised, since 2011. All these children should have had their homes remediated and been considered for chelation therapy, but they were not, as ZCCM-IH was no longer funding chelation, and there was no ongoing cleanup effort.[141]
Catherine’s parents moved to Kabwe almost two decades ago, after her father left his mining job in the Copperbelt, an adjacent province. With her husband out of work, Catherine’s mother Rebecca developed a business selling tomatoes and vegetables. Catherine is a 2nd grader at a private school in an affected township. Eight years old now, she was tested as a toddler in 2012 and re-tested sometime after. Her mother did not remember her original lead level but said she was Class 4 when re-tested. Catherine was given soya and milk the first time she was tested and blood tonic the second time.[142]
Jean, 8, was tested in 2012 at age two and found to be Class 4. ZCCM-IH gave her milk and soya. Her 32-year-old mother, Cynthia, was told not to let her play in the dirt, to wash her hands before eating, and to change her clothes when she came inside. When Cynthia took her daughter to the health center, she said they would only provide Panadol and advise her to go to the general hospital. Jean had never made it to the hospital, Cynthia said, because the family could not afford to pay for care.[143]
James, 7, was tested in 2014 and found to be Class 5. ZCCM-IH gave him milk and soya. His mother said he has headaches, stomach pain, and weakness.[144]
Limited and Irregular Provision of Nutritional Supplements
In the years since the CEP ended, children under 7 who were found to have elevated lead levels were given either milk and soya or a vitamin syrup called Vard’s Blood Tonic—or a combination of both. Vard’s is a vitamin syrup containing Iron, Vitamin C, and B-Complex, intended to counteract anemia, which can be both a cause and effect of increased lead absorption. After the initial provision, distribution of nutritional supplements was erratic or eventually ended, according to Human Rights Watch interviews.[145]
Parents or guardians for more than 40 children told Human Rights Watch that their children initially received milk, soya, and/or blood tonic in response to elevated blood lead levels. Some families reported being given nutritional supplements when they were first tested that were discontinued without being told why.
Nine-year-old Melody, a 3rd grader at a public school, said she enjoys playing the game waida, a form of jump rope, in her neighborhood. She and her brother, 13, were found to be Class 3 in 2012. Today Melody has stomach pain. She and her brother have memory problems. “You can send them to bring you plates,” their mother said. “They give you pots.” They were both given blood tonic initially but later stopped receiving it.[146]
Maria, 9, was tested in 2013 and found to be Class 4. She was given milk, soya, and another medicine in a bottle. After the initial provision, she only received milk or soya once every year or two. There should be regular check-ups for testing and treatment, her mother said. She observed that Maria receives nothing now.[147]
Other families reported only receiving nutritional supplements sporadically after their children were tested.[148]
Jane, 7, was tested in 2012 as a baby and found to be Class 5. At the time, her weight had been decreasing, and she looked thin. Her mother said she was given blood tonic, milk, and soya. The blood tonic provision stopped, but Jane still got milk and soya, although it was erratic, coming every three to six months. Jane’s mother said she wanted the government to resume providing blood tonic. She asked when the government would come to help children who were affected by lead.[149]
ZCCM-IH advised parents to buy milk and soya themselves, but some parents and guardians told Human Rights Watch they could not afford to buy these items regularly or at all.[150]
Alice, 12, the oldest of four siblings, said she wanted to be a lawyer when she grew up but added: “I do not learn well.” Alice was tested in 2012 and found to have elevated lead levels. She was given nutritional supplements, but her grandfather said they were not enough: the family only received one packet of milk and one packet of soya per month for her. He told Human Rights Watch, “The government has done very little about it [the lead exposure].” He added that the family struggled to afford soya and milk, as he had left his job in 1998.[151]
Failure to Track Lead-Related Hospitalization or Death
Although there are limited records of children’s hospitalization and death from lead poisoning in the early 1970s, there are no recent records. Zambia’s Health Management Information System (HMIS), a national health database, does not track such cases, and local health authorities have not set up any parallel system to collect and analyze data on lead poisoning.[152]
Human Rights Watch interviewed one mother whose son had extremely elevated lead levels at age 4 and died four years later, but there was no way to determine whether lead exposure played any role in his death.[153]
A hospital staff member in Kabwe said that at the hospital, lead poisoning was the last thing on people’s minds. He was not sure of any cases where a child died from lead poisoning. He said it would be helpful if the health system tracked it, such as through a register like the hospital has for tuberculosis, cancer, malaria, or HIV. He observed:
I’ve never attended a meeting about lead poisoning. Never ever…. It’s hard when you’re not tracking. Your index of suspicion is not that high…. It’s absent in our documents. It’s just not there.[154]
Necessity of Inclusive Education for Children with Disabilities or Learning Barriers
Lead poisoning can impair cognitive development, resulting in problems with concentration, memory, and learning. Parents, grandparents, teachers, and education officials told Human Rights Watch that children in Kabwe struggled with these very problems.
The 2012 Persons with Disabilities Act of Zambia requires the government to ensure that persons with disabilities receive inclusive education, reasonable accommodation, “the support required, within the general education system, to facilitate their effective education,” and “effective individualised support measures … in environments that maximise academic and social development, consistent with the goal of full inclusion.”[155] Reasonable accommodations can include allowing a student more time, reducing levels of background noise, or employing a qualified learning support assistant for one or more students. This applies to all children with disabilities—whether or not they are proven to be connected to lead.
However, both an official at the Ministry of General Education and members of an education-focused NGO in the capital told Human Rights Watch that the national government is currently doing little to improve education for children with disabilities or learning barriers.[156]
A representative of the District Education Board and members of the District Assessment Centre in Kabwe explained how the screening process for disabilities is expected to work. If a parent or guardian suspects a child has a disability, the school usually conducts an assessment through the guidance counselor, teacher, or deputy headteacher. If the school personnel believe a child may have a disability, they refer the parents or guardians to the District Assessment Centre. The District Assessment Centre refers the child to a psychologist at Kabwe General Hospital for an assessment, which forms the basis of an application for accommodations and individualized support measures in education.[157]
Headteachers at two public schools in Kabwe and several other teachers told Human Rights Watch that they had a high number of “slow learners,” a term used to loosely describe children who face challenges learning but do not necessarily have a learning disability.[158] The education authorities in Kabwe told Human Rights Watch that they had seen children who showed lack of concentration, hyperactivity, and difficulty with memory.[159] A special education teacher said that difficulty remembering particularly affected children with whom he worked.[160]
However, despite the prevalence of increased lead levels in Kabwe, education authorities said they were not routinely testing children with concentration and memory issues for lead levels. They assumed that lead exposure had caused learning barriers and disabilities but could not recall any cases in which they had requested lead tests.[161]
Some headteachers and teachers described their efforts to support children experiencing learning barriers.[162] One public school headteacher said that his school sought to assist students experiencing learning barriers through additional support within the classroom and outside, individual attention, and involvement of parents. However, he also acknowledged that tuition was required for extra lessons.[163]
Human Rights Watch spoke to the parents and guardians of a number of children who had been tested and found to have elevated lead levels and who faced challenges in school because of poor memory, inability to focus, or slower pace when learning. Some said that their children did not receive accommodations in school to address these problems.
Chikulu and Kapya, 8-year-old twin boys, were tested for lead in 2014 and found to have elevated levels. They are in the 4th grade at a public primary school. According to their grandfather, both are not doing very well in class. They are far behind grade level academically, and they fight a lot. They have difficulty concentrating and have been described by their teacher as “slow learners.” Their grandfather attributed the lack of support to school over-enrollment: class sizes were too large, leaving insufficient room for individualized attention. The school leaders and teachers were aware of the lead issue, he said, but did not really raise or address it.[164]
George, 10, who was found to have elevated lead levels in 2014, is in 2nd grade at a public primary school. His mother said:
He wasn’t born like this. He was sharp. But over time his behavior changed. It started around the age of 4…. When I get the report, the school says he is brilliant, but he is slow. It takes him time to come out with answers, also written answers.
She said the school does not give him more time in class. She has not told his teachers about his elevated lead levels.[165]
Thelma, 11, was tested in 2010 and found to have elevated lead levels. She is in the 5th grade at a public school. Her grandfather said that she has poor results in school. He has not told the school about his daughter’s past lead levels. He said:
Once I went to school at the end of the term after we received report cards, their mistress told me that concentration is a bit of a problem for the girl…. What we believe is that they [teachers] are not concerned.
He attributed the inaction by the school on his granddaughter’s learning needs to the high number of students per class and added that the extra tuition is required for special assistance, something the family cannot afford, although under law it should be free.[166]
The government should deepen its efforts to address lead-associated disabilities or learning barriers in light of the reality of widespread lead poisoning in Kabwe. Schools should ensure that they adequately respond to the needs of many children facing learning disabilities or barriers potentially connected to lead poisoning, and that they provide accommodations and individual learning support accordingly.
In response to these findings, the Ministry of Mines and Minerals Development stated in a letter to Human Rights Watch that the government’s new World Bank-funded project had engaged the Ministry of General Education to train teachers and other community members on how to detect signs and symptoms of lead poisoning in children. The government in the letter said that going forward, it would ensure that the needs of pupils affected by lead poisoning would be addressed and that they would not be subjected to the same examination assessment methods as other children.[167]
Further Health Threats from Mining and Mineral Waste Processing Plans at the Former Kabwe Mine
Women in fact we are not supposed to be here. There is a lot of energy we are wasting here. If the government could find something to do for us. We are here because we have nothing to do at home. There is no industry in Kabwe.
—Woman, Miner, Kabwe, November 2018[168]
I don’t like the work here, but it is the only thing I can do.
—Man, Miner, 35, Black Mountain, Kabwe, November 2018[169]
Twenty-five years after the closure of the Kabwe mine, its waste dumps remain in place. No meaningful work has been undertaken to remove the source of the contamination. Lead dust from the uncovered waste dumps continues to blow over to nearby residential areas and threaten community health.
The government has not conducted a remediation or reclamation (land restoration) program and has recently issued several licenses for small-scale mining. Small-scale mining at the former mine site produces risks to residents’ health by creating another pathway for exposure to lead dust.
The government has also granted a large-scale mining license for much of the former mine area to a company that plans to recover lead, zinc, and vanadium from the waste. Waste processing, if not carefully managed, carries the risk of creating further problems for human health and the environment by generating additional dust and polluting the water.
Health Risks from the “Black Mountain” and Other Lead Waste at the Former Mine Site
The former mine area contains over three million tons of tailings (waste from the mining process), about 2.5 million tons of slag (waste from the smelter), and other waste.[170] The most visible waste dump is a large, dark pile of slag, locally known as the “Black Mountain because of its dark color. While the lead content in different kinds of waste varies,[171] every kind of lead waste poses risks to human health and the environment.[172]
After the 1994 closure of the mine, ZCCM issued a Kabwe Mine Site Rehabilitation and Decommissioning Plan in 1995 to address its environmental legacy. Over the next two years, ZCCM began to cover the tailings dumps (mine waste) with coarse, granular slag to reduce windblown lead dust. However, a World Bank-funded environmental assessment found in 2002 that those measures were “incomplete because of financial constraints.”[173]
The government’s strategy document for remediation does not include an assessment of remediation or reclamation options for the defunct Kabwe mine, such as capping (sealing) or removing the mine’s waste piles, both practices employed elsewhere to remediate contaminated sites, for example in the United States, Canada, and Ghana.[174] The government has, however, acknowledged problems with the “overall management of environmental liabilities” in Kabwe and other mining areas.[175]
In 2012, the government issued a large-scale mining license covering over seven square kilometers to a British company called Berkeley Mineral Resources (BMR). With the license, the company acquired the Kabwe tailings stockpiles as well as all other mined resources or unmined resources at the former mine, meaning they gained access both to waste produced during previous mining and to raw materials that had not yet been mined.[176] At the same time, ZCCM-IH retained historical liabilities, shielding BMR from legal liability for existing environmental damage.[177] In addition, BMR’s subsidiary Enviro Processing Limited (EPL) obtained a small-scale mining license in 2011.[178] According to EPL, two small-scale mining licenses have also been granted by the government.[179]
The government has opened the door for further mining and mineral waste processing, but it has not addressed the legacy of contamination.
How Have Lead Mines Been Cleaned Up Elsewhere?Some of the more effective examples of mine cleanup come from the United States, although the resources available for cleanup in Zambia are not comparable. The United States has many historic mining sites and a massive contamination problem as a result. Bunker Hill, Idaho, in the northwestern US, was an important site for lead, silver, zinc, and other metal mining, as well as smelting, until the 1980s. As a result of the pervasive lead pollution, children’s blood lead levels were found to be elevated. To clean up Bunker Hill, a government-funded program was launched in 1983. At the industrial complex itself, measures included capping of waste, removing of waste, demolition of processing facilities, revegetation efforts, treatment of contaminated water, and drainage improvements. Outside the immediate industrial area, the program included the clean-up of residential areas, health promotion, and lead monitoring.[180] The remediation program enabled ecological restoration, such as the creation of a wetland habitat, but had limitations, too. For example, the most intensive reclamation activities only focused on a narrowly defined area, excluding other affected populations, including indigenous people.[181] |
Health Risks of Small-Scale Mining
Since its closure in 1994, small-scale mining has become the main activity at the former Kabwe mine. Artisanal and small-scale mining, that is, mining with little or no machinery, has been taking place in the absence of one central mining company.
Small-scale mining for lead poses severe health risks and affects children in Kabwe twofold. First, children risk getting exposed to particularly high levels of lead when adult family members work at the mine and return home with lead on their body, clothes, tools, or shoes. Second, older children themselves work at the mine.
Small-scale mining is an important economic sector in Zambia and many other countries across the globe, but small-scale mining for lead is rare.[182] While the government has issued some licenses for mining, there are also unlicensed, illegal mining operations.
When Human Rights Watch visited the mine area, adult men, adult women, and a few older boys were working at several spots, including the “Black Mountain” and another area they called the “Savage Mountain.” They dug up the soil and rocks, placed them in bags, and carried them to collection places or buyers. Some would wash the rocks to sift out certain minerals. Miners said they were mining for zinc and lead, as well as rock material called dolomite and the lead ore galena, and explained that other tasks including crushing rocks and selling the mined material to buyers.
Most adults working at the mine were aware that lead is dangerous and tried to take steps to protect themselves, their children, and other relatives.
Margaret, a mother of three, who worked at the “Savage Mountain,” told Human Rights Watch that she washed and changed clothes when she got home. Still, she worried about lead.[183] Other women and men working at the mine had the same practice of using a set of clothes for mining—sometimes leaving them at the mine site—and then bathing after returning home from the mine. Some would first bathe in the pools of water at the mine site, change clothes, and then repeat the process at home. Some said they drank milk to limit lead absorption and gave milk to their children.

In their current form, these safety measures are unlikely to eliminate the risks to miners or their children. The miners are still exposed to lead dust while they work, and the lack of proper washing facilities near the mine site means they will not be able to remove all lead dust from their bodies, hair, clothes, shoes, and other items, such as bags.
Several women miners expressed the desire to do other work instead of mining. Margaret told Human Rights Watch she did not like working at the mine and would prefer to have a business selling things at markets.[184] Similarly, Brenda, who has a 10-year-old daughter, said she would like to start any kind of business that would allow her to “move out of this place.”[185] Another woman said she felt the work was very bad, very dangerous, and tiresome.[186] Several women called upon the government to provide funds for alternative livelihoods. Other miners felt they had no choice but to work at the mine.[187] Evans, a father of three, told Human Rights Watch, “I don’t like the work here, but it is the only thing I can do.”[188]
Some adult miners started working at the mine when they were under the age of 18 and still in school. After school hours, they worked at the mine to pay school fees.
Mubanga, 18, said he started working at the mine when he was 17. He had stopped going to school in 9th grade. His job was to dig four-meter holes, and he expressed concern about lead, particularly what he described as its effect on the brain, adding that he would change his clothes, wash, and drink milk to protect himself. He said many boys under the age of 14 work at the mine site.[189]
Human Rights Watch also spoke to three older boys working at the mine site.
Isaac, a 17-year-old boy living with his grandmother in Kabwe, said he started working at the mine at age 12. At first, he combined work and school, working in the morning and attending school in the afternoon. However, he dropped out after the 9th grade because he could not pay school fees. Isaac said that he sometimes had stomach pains so severe that he could not sleep at night. He had never been tested for lead.[190]
Peter, a 17-year-old orphan, said he had been working at the mine site for about 10 years. He attended school until the 8th grade and then dropped out. Peter did not have any protection from the hazards of the mine site, but he bathed when he could because he heard that would help protect him against the effects of lead. He said he experienced appetite loss, constipation, and issues with his eyes, which may or may not be a result of lead poisoning. He said he wished the government could provide him with another option for work.[191]
Wankumbu, 16, who had just started work at the mine site three days before Human Rights Watch interviewed him, said his job was lifting and carrying bags. He had stopped going to school the previous year, when he was in 7th grade.[192]
Human Rights Watch interviews confirmed that adult and child small-scale miners in Kabwe work in hazardous conditions. Although the Kabwe Municipal Council staff have gone to the mine site to teach the miners about safety, most miners are working without adequate precautions to protect themselves or their families from lead exposure.[193] It is therefore a positive sign that the Zambian government has expressed an interest in ending unlicensed small-scale mining at the old mine site and that its latest World Bank-funded project includes plans to develop alternative income-generating activities for community members.

If mining is to continue, however, the government should ensure that operations are licensed, regularly monitored, and only conducted in accordance with mining regulations and law. According to national law, small-scale mining licenses can only be granted when a project brief or environmental impact assessment has been approved by the Zambia Environmental Management Agency as “not likely to cause adverse effects on the environment.”[194] Mining operations are not allowed to create an unsafe working environment or uncontrollable pollution of the area.[195]
In its letter to Human Rights Watch, the Ministry of Mines and Minerals Development acknowledged that illegal mining operations by artisanal and small-scale miners continued to be a major challenge across the country and had become more pronounced in former mining areas like Kabwe. The letter stated that the government would continue to monitor all mining operations and carry out routine inspections to ensure that operators were licensed and compliant with relevant law. It also stated that the new World-Bank-funded government project would include livelihood interventions “to discourage vulnerable persons, especially women and youths, from engaging in income generation activities which promote pollution.”[196]
Health Risks Related to Waste Processing Plans by Berkeley Mineral Resources and Jubilee Metals Group
Current plans to process the mineral waste at the former Kabwe mine pose further risks to human health and the environment. Two independent experts told Human Rights Watch that the environmental impact assessment for these plans that does not adequately address some of these serious risks.
In 2015, EPL—a subsidiary of Berkeley Mineral Resources (BMR)—submitted an environmental impact statement to the Zambia Environmental Management Agency, the government agency that oversees environmental issues. The company stated that it was planning to clean up the former Kabwe mine by removing lead and zinc from the tailings through chemical processing.[197] Waste processing carries the risk of creating further problems for human health and the environment by generating additional dust and polluting the water.[198]
The Zambian government approved the environmental impact statement in May 2016.[199] Human Rights Watch interviewed two independent experts on mine tailings for an assessment of EPL’s environmental impact statement. Ann Maest is a geochemist and Chief Scientist with E-Tech International, a non-profit that provides environmental technical support to communities on potential environmental impacts of large development projects.[200] Stu Levit is a land reclamation specialist working with the U.S.-based Center for Science in Public Participation, which describes its mission as “providing objective research and technical advice to people impacted by mining.”[201]
Both experts concluded that EPL’s proposal failed to demonstrate how any harmful impacts of the proposed reprocessing activities would be prevented or mitigated.[202] In particular, they concluded that the environmental impact assessment lacked vital information and baseline data on the composition of the tailings, the existing water and air quality, and other factors, resulting in an inconclusive and poor assessment of environmental and health risks.[203] For example, they argued that EPL’s claim that its actions “will not result in water pollution” was not supported by facts, as there were water sources nearby.[204] And even though EPL recognized the risk of dust emissions from its operations, the experts found the measures described to address these inadequate, as they lacked detail on how the company would suppress dust in different weather conditions and seasons, and failed to consider the use of manganese for effective dust suppression.[205] The experts also found that the environmental impact statement had a poor post-closure plan: It proposed only five years of post-closure monitoring, when a recent mining standard set the goal to be 25 years, and it did not include a reclamation plan.[206] According to E-Tech International, “a much more robust and less biased evaluation of the potential adverse effects of the project should be required in a revised EIS for the project carried out by Jubilee Metals.”[207]
In 2018, Jubilee Metals Group, a South African company, entered into a joint venture with BMR. As designated sole operator of the project, Jubilee Metals reviewed and changed BMR’s plans by, among other things, opting to separate the zinc and lead recovery processes and proposing a method to recover the highly valuable metal vanadium as well.[208] In March 2019, Jubilee Metals announced that it had bought a refinery right next to the former Kabwe mine for zinc processing, and that it anticipated producing metal within one year.[209]
Human Rights Watch spoke with BMR and Jubilee Metals and wrote both companies, requesting further information on how they planned to address the environmental and health risks of these operations. BMR responded by referring Human Rights Watch to Jubilee. Jubilee did not respond.
In April 2019, representatives of the Zambia Environmental Management Agency (ZEMA) told Human Rights Watch they had recently met with Jubilee Metals to discuss its proposed Kabwe project and instructed Jubilee to submit a new environmental impact assessment before commencing operations.[210]
Any future waste processing project should be carefully scrutinized by the government for potential human rights and environmental impacts. The government should only allow Jubilee Metals to move forward if the company demonstrates that it has identified, and has sufficient plans in place to mitigate, any human rights risks posed by its operations.
In its letter to Human Rights Watch, the Ministry of Mines and Minerals Development recognized the risks associated with the re-mining and reprocessing of mineral waste in Kabwe. It further acknowledged that if mining activities were not strictly monitored, lead could be reintroduced to the surrounding communities, which could reverse the government’s remediation and health interventions and constitute a waste of public resources. The letter stated that the government would ensure that the new mining operations would not reverse the progress made.[211]
III. Government Plans: Remediation, Testing, and Treatment
Reduce this lead here in Kabwe. They should bring us medicine and continue to support us with milk and soya so we don’t have lead in our bodies.
—Boy, 13, Kabwe, November 2018[212]
In December 2016, the Zambian government launched a five-year World Bank-funded project, the Zambia – Mining and Environmental Remediation and Improvement Project (ZMERIP). Unlike the Copperbelt Environment Project (CEP), the new project includes the Kabwe Municipal Council as a key stakeholder to ensure that the project’s gains are sustained when the World Bank funding ends. Both the Zambian government and the World Bank informed Human Rights Watch they incorporated this change in the project design in response to lessons learned from the CEP.[213] Key stakeholders at the national level include the Ministry of Mines and Minerals Development and the Zambia Environmental Management Agency (ZEMA). Project fund have been disbursed to these three entities.[214] The project offers the government an important opportunity to address the ongoing legacy of the Kabwe mine.
Human Rights Watch is concerned, however, that the project will not address the full scope of lead poisoning and contamination. Over two years after its launch, the project remains in the planning stages, in part a result of bureaucratic delays relating to secondment (the temporary reassignment of officials to new, project-related positions) and project restructuring. Officials in the Ministry of Mines and Minerals Development attributed the delays to several factors, including bureaucracy within both the Zambian government and the World Bank and the rules of public procurement.[215]
In response to the delays, the World Bank rated overall implementation progress “Moderately Unsatisfactory” in its June 2019 Implementation Status & Results Report.[216]
The delays, compounded by what some community members described as the government’s poor information sharing and community engagement, have caused frustration and distrust among residents. Zambian government officials and World Bank representatives told Human Rights Watch that the government intended to commence the remediation and health components of the project before the end of 2019.
Remediation
The program is slated to include a voluntary remediation program for homes and “hotspots” with high lead exposure.[217] In July 2018, the Kabwe Municipal Council issued a request for bids for the engineering design for the remediation program, suggesting that it would focus on households in Chowa and Kasanda as well as other “contaminated hotspots with lead-bearing material.”[218] The Council’s stated objective was to decrease soil lead levels in areas where surface soil lead concentrations were “routinely greater than 2,000 mg/kg.”[219] At time of writing, the company that will design the remediation program had not yet been appointed.[220]
The remediation program is also intended to improve the drainage and flow of the Kabwe Canal, which was used to discharge mine waste when the mine was still operational. The canal, which annually becomes clogged with weeds and debris and then floods during the rainy season, was cleaned under the CEP but not maintained after. The program also includes plans to upgrade the Kabwe solid waste dump site so it can serve as a repository for contaminated material from residential areas.[221]
Given the failure of the CEP to reduce soil lead levels in Kabwe’s affected townships, the new project should adopt a more effective remediation approach. The new remediation design should be both comprehensive and sustainable enough to ensure a lasting solution.
The government officials managing the project were unsure whether the new remediation plan would address the full extent of residential contamination.[222] Only the townships of Chowa, Kasanda, and Makululu were mentioned in the government’s most recent request for bids on the remediation design.[223] Previous studies have found high levels of contamination in other townships as well, including Makandanyama and Mutwe Wansofu. Additionally, children in the townships of Waya, Katondo, and Railway have also been found to have elevated blood lead levels.[224]
Government officials were also unsure whether the remediation of contaminated hotspots would examine or address the full scope of the contamination in public areas, such as schools, play areas, or health centers.
Officials at both the Ministry of Mines and Minerals Development and the World Bank told Human Rights Watch that, as a result of budgetary constraints, the project would not pave roads, despite the contamination risks posed by road dust.[225]
In its letter to Human Rights Watch, the Ministry of Mines and Minerals Development stated that engineering designs and Environmental and Social Impact Assessments (ESIAs) would be undertaken “to bring out the best possible options which then could be implemented to address lead exposure in homes, schools, health centres, roads and open play ground within the affected area.” The letter emphasized, however, that comprehensive remediation in Kabwe and other areas of the country would require substantial financial resources that Zambia does not currently have, and in particular, that the government does not have enough resources to clean up “open spaces and other public places in affected areas.” The letter stated that the government would “continue to mobilise resources to substantially reduce lead pollution.”[226]
Finally, the project does not address windblown dust from the open tailings dump.
Health
The project includes plans for testing and treating at least 10,000 children, pregnant women, mothers, and other individuals, which will be overseen by the District Medical Officer in Kabwe.[227] Children are meant to receive treatment in the form of chelation therapy or nutritional supplements, depending on their blood lead levels. As an improvement on the last project, children with blood lead levels of 45 ug/dL will be eligible for chelation therapy. Under the last project, only children with blood lead levels of 65 ug/dL and above received chelation. Without coordinated efforts to remediate, however, chelation will not be effective, a fact the World Bank notes in its project document: “Chelation therapy will only work with remediation (otherwise the population continues to live in a contaminated environment and ingest lead).”[228]
All potentially affected children should have access to testing and treatment. The government has not yet published information on the details of the testing program, including the age group targeted. The last project and the post-2011 continuation of the CEP program only tested and treated children below age 7. Children were no longer monitored after that point, despite ongoing exposure, and, in some cases, symptoms that correlated with lead poisoning. The Ministry of Mines and Minerals Development informed Human Rights Watch that the project would work with other local initiatives to retest and treat children previously found to have elevated blood lead levels.[229]
In its letter to Human Rights Watch, the Ministry of Mines and Minerals Development stated that the Ministry of Health planned to integrate lead screening and procurement of medicines and other consumables into the main strategic plan for the health sector. This way, the letter said, new health interventions would “be sustained beyond the project life.”[230]
Human Rights Watch was unable to ascertain the specific plans under the new project for the treatment of adults, including pregnant or breastfeeding women or other women of childbearing age. Breastmilk alternatives (i.e., infant formula) would be advisable for women with elevated blood lead levels, so long as the government ensures that breastmilk alternatives are targeted and do not disturb general community norms around breastfeeding. Infants born to women with elevated blood lead levels may also require specialized care.
At time of writing, the testing and treatment regimen had not begun, and the Zambian government was still in the process of procuring chelation medicine through the United Nations Children’s Fund (UNICEF).[231] Officials from the Ministry of Mines and Minerals Development stated that the treatment campaign would commence with the first delivery of drugs in September 2019.
Human Rights Watch was unable to confirm that the government will ensure that chelation is preceded by remediation in the case of each child treated, given the delays in both components of the project. In November 2018, officials at the Ministry of Mines and Minerals Development told Human Rights Watch that they planned to execute the remediation and health components in parallel,[232] but the most recent procurement documents suggest that the remediation design is not scheduled to be finalized until two months after the chelation medicine is expected to arrive.[233]
Human Rights Watch reached out to the World Bank regarding the sequencing of chelation and remediation. The World Bank responded that they recognize the importance of closely linking chelation therapy to household dust suppression measures. However, they did not provide further clarity in their written response on their plans for the sequencing of initiatives.[234]
Human Rights Watch shared its concerns regarding the sequencing of chelation and remediation with officials in the Ministry of Mines and Minerals Development. In its letter, the ministry explained that the project had planned an “emergency response” before the end of 2019 to clean up select contaminated households where the first 145 affected children would be treated. The ministry pledged to fast-track the cleanup intervention to ensure that children would not return to a contaminated environment.[235]
The government should ensure that all treatment, especially chelation therapy, coincides with remediation; without remediation, patients will be re-exposed to lead as soon as they return home.
Community Engagement
It needs a lot of sensitization for people to understand it better. I strongly feel that we have a lot of things to do.
—Father, Kabwe, November 2018[236]
Some community members complained to Human Rights Watch that the government has not done enough to share information with and engage affected communities in Kabwe.
The project includes a plan to develop livelihood and income generation opportunities in contaminated areas to “enhance community involvement in addressing environmental health risks.”[237]
The project will also include education and awareness campaigns to sensitize schoolchildren in Kabwe about lead.[238] According to the Ministry of Mines and Minerals Development, the government has begun a “robust sensitisation campaign” in select schools in lead-affected communities to provide information on lead poisoning.[239]
Some community members in Kabwe told Human Rights Watch they knew little about the progress of the new World Bank-funded project or were not aware of the project at all.[240] The father of a young child said that he had heard of the project but did not know whether the government had yet received funding for it.[241]
Members of a local Ward Development Committee in a lead-affected area observed that a lot of money was coming from the World Bank, but they expressed concern at the process, which they said was not transparent. They also raised concerns over the lack of consultation, that they were only invited to the launch, and that two years after the project was launched, materials have not been procured, and contractors not selected. They said that the Kabwe Municipal Council did not update them, and the community lacked confidence in the Council.[242] Another Ward Development Committee in a contaminated area called for better community education and outreach from the World Bank and local authorities.[243]
An NGO staff member also expressed concern about what he described as a lack of consultation. He outlined one way the government could learn from the previous World Bank-funded project, saying of the CEP: “I strongly feel that it should have started from the grassroots going upward.” He called for community ownership of the new project, stressing that community members should be involved and should benefit from the money spent.[244]
Community involvement will be crucial to ensure the project’s gains are long-term. The government should include community members in the planning and execution of all components of the project.
IV. Zambia’s Domestic and International Obligations
Right to Health and Health Information
The right to the highest attainable standard of health is guaranteed by international treaties to which Zambia is a party, including the International Covenant on Economic Social and Cultural Rights (ICESCR), the Convention on the Rights of the Child (CRC), and the African Charter on Human and Peoples’ Rights.[245]
The Committee on Economic, Social and Cultural Rights (CESCR), the treaty body which interprets state obligations under the ICESCR and monitors state compliance with its provisions, has held that social determinants of health are crucial to the full realization of the right to health, including “healthy occupational and environmental conditions, and access to health-related information and education.[246]
According to the CESCR, a state party cannot, under any circumstances, justify its non-compliance with core obligations, which are non-derogable.[247] The core obligations defined by the committee include providing essential drugs.[248] Chelation medicine, included on both the WHO Model List of Essential Medicines and the WHO Model List of Essential Medicines for Children, should be seen as one such essential drug.[249] The government should include it on its own list of essential medicines and take immediate steps to ensure its availability.
Obligations of “comparable priority” to core obligations include maternal and child health and providing appropriate training for health personnel, and the provision of health education and access to health information.[250]
Right to a Healthy Environment
The Environmental Management Act of 2011 in Zambia guarantees “the right to a clean, safe and healthy environment.” It also states that “the citizen shall have access to environmental information to enable the citizen make informed personal choices which encourages improved performance by industry and the Government.”[251] This guarantee largely echoes the development of international human rights standards, and should be interpreted by the government in light of those standards.
In March 2018, the Special Rapporteur on human rights and the environment presented to the Human Rights Council a set of framework principles on human rights and the environment. The Special Rapporteur explained that the Framework Principles “set out basic obligations of States under human rights law as they relate to the enjoyment of a safe, clean, healthy and sustainable environment.”[252] Framework principle 1 calls on states to “ensure a safe, clean, healthy and sustainable environment in order to respect, protect and fulfil human rights.” [253]
The ICESCR requires that states, in order to realize the right to the highest attainable standard of health, take the steps necessary for “the improvement of all aspects of environmental and industrial hygiene.”[254]
The CECSR has clarified that this right imposes on states:
The requirement to ensure … the prevention and reduction of the population’s exposure to harmful chemicals or other detrimental environmental conditions that directly or indirectly impact upon human health….
States are also required to adopt measures against the environmental and occupational health hazards and against any other threat as demonstrated by epidemiological data. For this purpose they should formulate and implement national policies aimed at reducing and eliminating pollution of air, water and soil, including pollution by heavy metals such as lead from gasoline.[255]
States should also refrain from unlawfully polluting air, water and soil e.g. through industrial waste from State-owned facilities.[256]
The CESCR has also explained that governments are also obligated to take steps to prevent violations of the right to ICESCR rights, including the right to health, by private actors:
Violations of the obligation to protect follow from the failure of a State to take all necessary measures to safeguard persons within their jurisdiction from infringements of the right to health by third parties. This category includes … the failure to enact or enforce laws to prevent the pollution of water, air and soil by extractive and manufacturing industries.[257]
The Committee on the Rights of the Child, the treaty body which monitors compliance with the Convention on the Rights of the Child, when describing the right of the child to the enjoyment of the highest attainable standard of health, calls on states to take appropriate measures “to combat disease and malnutrition … taking into consideration the dangers and risks of environmental pollution.”[258] Relevant regional human rights instruments—such as the African Charter, and its Additional Protocol on the Rights of Women—also recognize the right to live in a healthy and sustainable environment.[259]
The African Commission on Human and Peoples’ Rights has stated:
Government compliance with the spirit of Article 16 and Article 24 of the African Charter must also include ordering or at least permitting independent scientific monitoring of threatened environments, requiring and publicising environmental and social impact studies prior to any major industrial development, undertaking appropriate monitoring and providing information to those communities exposed to hazardous materials and activities and providing meaningful opportunities for individuals to be heard and to participate in the development decisions affecting their communities.[260]
Right to Education
The Convention on the Rights of Persons with Disabilities (CRPD), to which Zambia is party, calls inclusive education “a fundamental human right of all learners.”[261] An inclusive education system should focus on “the full and effective participation, accessibility, attendance and achievement of all students” in the ordinary school system.[262] The education system should provide a personalized educational response and “flexible curricula, teaching and learning methods, which requires support and reasonable accommodation so that learners are able to fulfill their potential.”[263]
Accommodations for pupils experiencing learning barriers or learning disabilities may include changing the location of a class, providing different forms of communication and learning materials in alternative/accessible formats, or providing students with a note-taker. Provision of non-material accommodations, such as allowing a student more time, reducing levels of background noise, sensitivity to sensory overload, alternative evaluation methods or replacing an element of curriculum by an alternative element, should also be considered. Support can also consist of a qualified learning support assistant, either shared or on a one-to-one basis, depending on the requirements of the student.[264]
Right to Play
Article 31 of the CRC guarantees “the right of the child to engage in play and recreational activities appropriate to the age of the child.”[265] The Committee on the Rights of the Child has stated:
Children have a spontaneous urge to play and participate in recreational activities and will seek out opportunities to do so in the most unfavourable environments. However, certain conditions need to be assured, in accordance with children’s evolving capacities, if they are to realize their rights under article 31 to the optimum extent.[266]
One of these conditions, the Committee has found, is “An environment sufficiently free from waste, pollution, traffic and other physical hazards to allow them to circulate freely and safely within their local neighbourhood.”[267]
Occupational Health and Child Labor
The ICESCR requires that states, in order to realize the right to the highest attainable standard of health, shall take the steps necessary for the “prevention, treatment and control of … occupational and other diseases.” In addition, article 7 of ICESCR recognizes “the right of everyone to the enjoyment of just and favorable conditions of work” including “safe and healthy working conditions.”[268] The CESCR has affirmed states’ obligations to protect the health of its workers.[269]
The International Labour Organization (ILO) has developed a comprehensive body of conventions that address virtually every aspect of workers' rights. ILO Convention 161 specifically addresses workers occupational health and safety. Article 12 states: “The surveillance of workers' health in relation to work shall involve no loss of earnings for them, shall be free of charge and shall take place as far as possible during working hours.”[270] Article 13 states: “All workers shall be informed of health hazards involved in their work.”[271]
Zambia has ratified international and regional instruments concerning children’s rights and child labor, including ILO Convention 182 (the Worst Forms of Child Labour Convention), ILO Convention 138 (Minimum Age Convention), and the CRC.
The Worst Forms of Child Labour Convention prohibits the worst forms of child labor, including “work which, by its nature or the circumstances in which it is carried out, is likely to harm the health, safety or morals of children” (also known as hazardous work).[272] As a state party to the Worst Forms of Child Labour Convention, Zambia is obligated to take immediate and effective steps to ascertain what forms and conditions of child labor violate the convention and then prohibit and eliminate them.[273] The Convention obliges member states to take immediate action to prevent children from engaging in the worst forms of child labor; and to provide direct assistance for the removal of children engaged in the worst forms of child labor.[274]
Although the ILO does not maintain a list of occupations that in its view constitute hazardous work for children, ILO Recommendation No. 190 (the Worst Forms of Child Labour Recommendation) provides guidance to countries on determining what types of work constitute harmful or hazardous work for children.[275] Each state party is required to take this guidance into consideration as part of their efforts to identify specific tasks and occupations that constitute hazardous work for children.[276]
Zambia is also a party to the ILO Minimum Age Convention, which sets the basic minimum age for employment at 15, and states that children ages 13 to 15 may participate only in light work that is not likely to be harmful to their health or development or hinder their education.[277] The Minimum Age Convention also prohibits children under 18 from engaging in hazardous work.[278]
Zambia has ratified the Convention on the Rights of the Child (CRC), which provides that children have a right “to be protected from economic exploitation and from performing any work that is likely to be hazardous or to interfere with the child's education, or to be harmful to the child's health or physical, mental, spiritual, moral or social development.”[279] Under the convention, governments must take appropriate legislative, administrative, social, and educational measures to protect children from exploitative and hazardous work, including by establishing a minimum age for employment, regulating the hours and conditions of children’s work, and providing for “appropriate penalties or other sanctions to ensure the effective enforcement” of such protections.[280]
Zambian law also prohibits hazardous child labor for children under 18.[281]
Business and Human Rights
Governments have a duty to protect human rights in the context of business activity, through effective regulation.[282] The United Nations Guiding Principles on Business and Human Rights, which the UN Human Rights Council endorsed in 2011, state that this “requires taking appropriate steps to prevent, investigate and redress such abuse through effective policies, legislation, regulations and adjudication.”[283] Governments also have a duty to effectively enforce that legal and regulatory framework once it is in place, to prevent abuse and ensure accountability and redress for abuses that do occur. Governments should also continually assess whether existing rules—and the enforcement of those rules—are actually adequate to the task of ensuring respect for human rights, and improve upon them if they are not.[284]
While governments have the primary responsibility to respect, protect, and fulfill human rights under international law, private entities, including businesses, also have internationally recognized responsibilities regarding human rights, including workers’ rights and children’s rights. The UN Guiding Principles on Business and Human Rights are widely accepted as a legitimate articulation of businesses’ human rights responsibilities. They specify that businesses should exercise human rights due diligence to identify human rights risks associated with their operations, take effective steps to prevent or mitigate those risks, and ensure that the victims of any abuses have access to remedies.[285]
The Guiding Principles also require businesses to report formally on human rights due diligence measures to provide transparency and accountability. Reporting should be “of a form and frequency that reflect an enterprise’s human rights impacts and that are accessible to its intended audiences,” and provide “information that is sufficient to evaluate the adequacy of an enterprise’s response to the particular human rights impact involved.”[286]
The CRC has maintained that “duties and responsibilities to respect the rights of children extend in practice beyond the State and … apply to private actors and business enterprises,” and that “all businesses must meet their responsibilities regarding children’s rights and States must ensure they do so.”[287] The committee has also noted that “voluntary actions of corporate responsibility by business enterprises, such as social investments, advocacy and public policy engagement, voluntary codes of conduct, philanthropy, and other collective actions, can advance children’s rights,” but that these actions “are not a substitute for State action and regulation of businesses … or for businesses to comply with their responsibilities to respect children’s rights.” Furthermore, the CRC has stated, “if children are identified as victims of environmental pollution, immediate steps should be taken by all relevant parties to prevent further damage to the health and development of children and repair any damage done.”[288]
Acknowledgments
This report was researched and written by Joanna Naples-Mitchell, fellow in the Children’s Rights Division of Human Rights Watch. Juliane Kippenberg, associate director of the Children’s Rights Division, Zama Neff, director of the Children’s Rights Division, and Susan Raqib, senior coordinator in the Children’s Rights Division, participated in the field research.
The report was reviewed by Juliane Kippenberg, who also conducted additional research; Dewa Mavhinga, Southern Africa director; Marcos Orellana, Environment and Human Rights director; Sarah Saadoun, researcher, Business and Human Rights Division; Jane Buchanan, deputy director, Disability Rights Division; Elin Martinez, researcher, Children’s Rights Division; and Joseph Amon, health and human rights consultant. Babatunde Olugboji, deputy program director, provided program review, and Chris Albin-Lackey, senior legal adviser, provided legal review. Brian Root, senior quantitative analyst, provided data analysis and prepared the graphics. Komala Ramachandra, senior researcher, Business and Human Rights Division, provided additional expertise and input.
The report was prepared for publication by Fitzroy Hepkins, administrative manager; and José Martínez, senior administration coordinator at Human Rights Watch. Additional production assistance was provided by Delphine Starr and Alex Firth, associates in the Children’s Rights Division.
Human Rights Watch would like to thank Mary Jean Brown, Bret Ericson, Jack Caravanos, Perry Gottesfeld, Stu Levit, Ann Maest, Sam Mutiti, Trevor Thompson, and others who shared their technical expertise.
We would like to thank NGO colleagues, government officials, company representatives, researchers, and experts who provided information for this report.
Most importantly, we are deeply grateful to the parents, grandparents, children, and other community members in Kabwe who shared their stories with us.
Appendix I: Zambian Government Response to Summary of Key Findings from Human Rights Watch
Background
The Zambian Government is taking a proactive and holistic approach to address the issues of mine related pollution across the country and has outlined a number of multi-sectoral interventions to deal with the issues of lead pollution in Kabwe. However, resources available under the current World Bank funded project cannot address all the issues of lead pollution in Kabwe.
Government recognises some of the challenges which arose during the implementation of the Copper belt Environment Project and has, this time around under the Zambia Mining and Environmental Remediation and Improvement Project (ZMERIP) taken care of some of the deficiencies. Critical institutions and other stakeholders such as local municipalities, the Ministry of Education and Ministry of Health have been brought on board to ensure sustainability of the current interventions. ZMERIP is correctly anchored in the Ministry of Mines and Minerals Development as the lead implementation agency.
The offtake of ZMERIP may have been delayed due to bureaucracies on both GRZ and the World Bank but Government is determined to move the Project into actual implementation. It is worthy noting that technical interventions require engineering designs and environmental clearances to obtain optimum interventions. In addition, GRZ is bound by rules of public procurement and cannot afford to bypass regulations which ensure transparency, cost effectiveness and value for money since the funds being handled under ZMERIP are public funds. This has tended to create the impression of the Project being slow which is not correct.
Environment
The Zambian Government will implement activities that will result in sustainable and comprehensive plans for addressing environmental, health and social impacts resulting from mining activities in Zambia. This will include the legacy issues of lead pollution in Kabwe. This would be achieved by implementation of ZMERIP activities inter alia the following:
- Review and Development of Technical and Financial instrument for Environmental and Social Sustainability of Mine Sites and Mine Closure Guideline;
- National Plan for Prioritization and Rehabilitation of Mine Waste facilities;
- Conservation Plan for Lukanga Swamp and Upper Kafue Basin;
- Development of Protocols and Regulations for Operationalizing Permanent Environmental Fund; and
- Development of Continuous Environmental Monitoring System.
The instruments and pieces of legislation which will be developed would be applied in improving regulation of the mining sector in Zambia. Government cannot ignore improvement of the policy and legislative framework as doing so would be waiting for similar cases of mine related environmental pollution to occur before finding solutions.
Further, engineering designs and Environmental and Social Impact Assessments (ESIAs) for voluntary in-situ remediation, construction of the engineered hazardous and non-hazardous sanitary landfill and the concrete lining of the Kabwe Canal will technically inform how earmarked ZMERIP interventions in Kabwe especially in identified hotspots will contribute towards reducing lead exposure.
The design and ESIA studies are meant to bring out the best possible options which then could be implemented to address lead exposure in homes, schools, health centres, roads and open play ground within the affected area and to identify the sources of lead. It is important to note that comprehensive remediation in Kabwe and other areas of the country requires substantial financial resources which Zambia does not currently have.
Education
The Zambia Mining and Environmental Remediation and Improvement Project (ZMERIP) has engaged the Ministry of Education to train Teachers and Safety Health Education and Nutrition Coordinators on Lead awareness and how to detect signs and symptoms of Lead poisoning in children. A robust sensitisation campaign has commenced in Kabwe with tours of selected schools in Lead affected communities to provide information about the symptoms and health habits hence the need to equip residents with basic information on Lead poisoning and symptoms. This will enable them to provide social-emotional support to pupils affected by Lead poisoning.
Most schools have provisions to accommodate children with special education needs but not specifically tailored for Lead disabilities. Going forward Government will ensure that the needs of pupils affected by Lead poisoning are addressed and that they are not subjected to the same examination assessment methods as other children.
Health
Government has recognised Lead contamination as a public health concern and is committed to including the matter in the mainstream health care system to reduce effects of Lead exposure on communities in affected parts of Kabwe. Ministry of Health plans to integrate Lead screening, procurement of medicines and other consumables into the main strategic plan for the health sector for easy tracking and treatment of people with elevated Blood Lead Levels (BLL). To this extent, the interventions being developed under ZMERIP will be sustained beyond the project life.
ZMERIP is working with other local initiatives to retest and treat children with elevated BLL. The project plans to test and treat at least 10,000 people including children and pregnant women from the lead affected areas.
Government through ZMERIP has planned an emergency response before 2019 year end to clean up select contaminated households where the first 145 affected children in Kabwe will be treated. Government will fast track the clean-up intervention to ensure that children do not return to a contaminated environment. This will be done to complement the treatment campaign which is expected to commence with the first delivery of drugs in Zambia in September 2019. Government will scale up the Blood lead level testing to include affected mothers and other persons.
In all instances Government will endeavour to clean up the environment either prior to or during treatment for lead. It is important to note that Government does not have enough resources to address the issues of lead contamination especially the local road network, open spaces and other public places in affected areas. Government will continue to mobilise resources to substantially reduce lead pollution.
Mining
Small scale mining activities have been taking place at old waste rock stockpiles in proximity to the old Kabwe Zinc/Lead mine. The waste dump (Black Mountain) on the eastern side of the Lusaka – Kabwe road, was licenced to Enviro – Processing Limited (EPL). EPL entered into an agreement with Jubilee Group of Metals to resume the operations in Kabwe aimed at commercial recovery of lead and zinc from the waste stockpile.
The Government of the Republic of Zambia (GRZ) recognises the risks which would be associated with revamping mining/processing of lead/zinc bearing material in Kabwe amid environment remediation and health intervention under way. If mining activities are not strictly monitored, there would be re-introduction of lead to the surrounding communities which would reverse GRZ interventions and result in waste of public resources. As a remedial measure, before operations resume, GRZ through, Zambia Environmental Management Agency (ZEMA) and Mines Safety Department (MSD) will ensure EPL prepares a full Environmental and Social Impact Assessment (ESIA). Government will ensure that emerging mining operations do not reverse the progress made in addressing issues of lead pollution in Kabwe. Government is engaging EPL to secure a firm commitment to complement its interventions in Kabwe.
While it is true that illegal mining operations by artisanal and small scale miners continues to be a major challenge across the country, it has become more pronounced in mining districts and former mining areas which includes Kabwe. Government will continue to monitor all mining operations for compliance and ensure that operators are licensed and compliant to relevant pieces of legislation. A combined team of licencing, inspection and monitoring authorities will routinely carry out inspections in Kabwe which will be aimed at establishing the compliance of all mining operations both small and large scale.
Livelihood interventions
Government through ZMERIP will implement livelihood and income generation support activities in selected towns of Kabwe, Kitwe, Mufulira and Chingola to discourage vulnerable persons, especially women and youths, from engaging in income generation activities which promote pollution and to offer alternative income sources.
This intervention is meant to complement other interventions stated here.
Glossary of Acronyms
BMR Berkeley Mineral Resources
CDC United States Centers for Disease Control and Prevention
CEP Copperbelt Environment Project
EPA United States Environmental Protection Agency
EPL Enviro Processing Limited
HMIS Health Management Information System
JICA Japan International Cooperation Agency
KAMPAI Kabwe Mine Pollution Amelioration Initiative
METS Misenge Environmental & Technical Services Limited
WHO World Health Organization
ZCCM Zambia Consolidated Copper Mines Limited
ZCCM-IH Zambia Consolidated Copper Mines Investment Holdings
ZEMA Zambia Environmental Management Agency
ZMERIP Zambia - Mining and Environmental Remediation and Improvement Project
Glossary of Terms and Abbreviations
|
artisanal and small-scale mining |
Mining with simple or no machinery, little investment, and a large workforce; often in the informal work sector. |
|
|
|
|
Black Mountain |
A large, dark pile of slag (mine waste) at the site of the former Kabwe mine, locally known as the “Black Mountain” because of its dark color. Now a site of small-scale mining. |
|
|
|
|
chelation therapy |
The most common treatment for lead poisoning. Chelation medicine attaches to lead and other heavy metals in the bloodstream, forming a compound that is then released in urine. The medicine can be administered orally or through injection. Only considered in cases of severe lead poisoning with lead levels greater than 45 μg/dL. Removes lead from the bloodstream to prevent further absorption into the organs and bones, but it cannot reverse all of the health effects of any lead previously absorbed. |
|
|
|
|
child |
Anyone under the age of 18. |
|
|
|
|
Class 1 |
Blood lead level between 0-9 μg/dL. (This classification system was used in Kabwe from at least 2007-2016.) |
|
|
|
|
Class 2 |
Blood lead level between 10-19 μg/dL. (This classification system was used in Kabwe from at least 2007-2016.) |
|
|
|
|
Class 3 |
Blood lead level between 20-44 μg/dL. (This classification system was used in Kabwe from at least 2007-2016.) |
|
|
|
|
Class 4 |
Blood lead level between 45-64 μg/dL. (This classification system was used in Kabwe from at least 2007-2016.) |
|
|
|
|
Class 5 |
Blood lead level greater than or equal to 65 μg/dL. (This classification system was used in Kabwe from at least 2007-2016.) |
|
|
|
|
dolomite |
A mineral which is often found in rock form. |
|
|
|
|
elevated blood lead level |
Blood lead level at or above the US CDC reference level of 5 μg/dL. |
|
|
|
|
galena |
Naturally occurring mineral form of lead sulfide, the most important ore of lead. |
|
|
|
|
geophagia |
Soil ingestion. May be practiced for health or cultural reasons, sometimes based on the belief that soil contains nutrients. |
|
|
|
|
hotspot |
Location where high concentrations of pollutants may expose the local population to elevated health risks. |
|
|
|
|
lead poisoning |
The absorption and toxic buildup of lead in the body, indicated by elevated blood lead levels. May or may not cause visible symptoms. |
|
|
|
|
ore |
A natural solid material from which valuable minerals, usually metals, can be extracted. |
|
|
|
|
reclamation |
Land restoration to a more useable or natural state. |
|
|
|
|
remediation |
The removal of pollutants or contaminants from the environment. |
|
|
|
|
“Savage Mountain” |
The name that miners and other residents of Kabwe have given a massive expanse of mine waste at the site of the former Kabwe mine that has become a site for small-scale mining. Distinct site from the “Black Mountain.” |
|
|
|
|
slag |
The glass-like material produced as a byproduct when metals are separated (smelted) from their raw ores. |
|
|
|
|
smelter |
A facility that extracts metals from their ores by applying heat. |
|
|
|
|
smelter fumes |
The gases, smoke, or vapors produced as byproducts from smelter operations (including heavy metals such as lead, released in the form of dust particles). |
|
|
|
|
tailings |
Waste product resulting from the processing of ores. Can be quite toxic because of residual hazardous minerals or from toxic chemicals added as part of the extraction processes. |
|
|
|
|
vanadium |
A highly valuable element and metal, used, for example, as steel additive to make steel more shock-resistant. |
|
|
|
|
μg/dL |
Micrograms/deciliter. |